If you've ever wondered, there are several types of headgear. The most common type is the cervical pull type. That's the one with the strap that goes behind your neck. Here is Dakota Fanning modeling her reverse-pull type headgear. This is less common and is usually used in kids with a Class III occlusion or at least ones where you are basically trying to stimulate the upper maxilla to grow forward. It is also known as a Delaire "facemask"; you can see why. Dakota has been giving an update to talk show hosts on her progress with her "Braces".
If you've ever wondered, there are several types of headgear. The most common type is the cervical pull type. That's the one with the strap that goes behind your neck. Here is Dakota Fanning modeling her reverse-pull type headgear. This is less common and is usually used in kids with a Class III occlusion or at least ones where you are basically trying to stimulate the upper maxilla to grow forward. It is also known as a Delaire "facemask"; you can see why. Dakota has been giving an update to talk show hosts on her progress with her "Braces".
Tuesday, December 26, 2006
Reverse Pull Headgear
If you've ever wondered, there are several types of headgear. The most common type is the cervical pull type. That's the one with the strap that goes behind your neck. Here is Dakota Fanning modeling her reverse-pull type headgear. This is less common and is usually used in kids with a Class III occlusion or at least ones where you are basically trying to stimulate the upper maxilla to grow forward. It is also known as a Delaire "facemask"; you can see why. Dakota has been giving an update to talk show hosts on her progress with her "Braces".
Sunday, December 24, 2006
Rudolph and Hermie the Elf Update
Here is a copy of a previous post of mine regarding North Pole News with additional information at the end of the post:
 News Flash! A soon to be dentist, Hermey (aka Herbie), an elf employed by Santa Claus at the North Pole, has saved Christmas. Evidently Santa’s trip was under threat of cancellation due to inclement weather. Santa was able to make the trip with the assistance of Rudolph the Red Nosed Reindeer. The little known behind the scenes efforts of Hermey made it possible for Rudolph to be available for the trip. The abominable snowman (Bumble) had evidently captured Rudolph and friends.
News Flash! A soon to be dentist, Hermey (aka Herbie), an elf employed by Santa Claus at the North Pole, has saved Christmas. Evidently Santa’s trip was under threat of cancellation due to inclement weather. Santa was able to make the trip with the assistance of Rudolph the Red Nosed Reindeer. The little known behind the scenes efforts of Hermey made it possible for Rudolph to be available for the trip. The abominable snowman (Bumble) had evidently captured Rudolph and friends.  With Rudolph unconscious, Hermey organized a rescue mission with Yukon Cornelius. Upon discovery of the bumble’s real problem, (bad teeth), Hermey with his dental skills, rendered the Bumble a gentle giant. Anesthesia services were provided by Yukon by droping a big rock on the Bumble's head. Rudolph returned unharmed to help guide Santa’s Sleigh! Once again showing the triumph of Dentistry.
With Rudolph unconscious, Hermey organized a rescue mission with Yukon Cornelius. Upon discovery of the bumble’s real problem, (bad teeth), Hermey with his dental skills, rendered the Bumble a gentle giant. Anesthesia services were provided by Yukon by droping a big rock on the Bumble's head. Rudolph returned unharmed to help guide Santa’s Sleigh! Once again showing the triumph of Dentistry.
Merry Christmas!
*Followup information on these events may be found here: What Ever Happenned to Hermie the Elf?
 News Flash! A soon to be dentist, Hermey (aka Herbie), an elf employed by Santa Claus at the North Pole, has saved Christmas. Evidently Santa’s trip was under threat of cancellation due to inclement weather. Santa was able to make the trip with the assistance of Rudolph the Red Nosed Reindeer. The little known behind the scenes efforts of Hermey made it possible for Rudolph to be available for the trip. The abominable snowman (Bumble) had evidently captured Rudolph and friends.
News Flash! A soon to be dentist, Hermey (aka Herbie), an elf employed by Santa Claus at the North Pole, has saved Christmas. Evidently Santa’s trip was under threat of cancellation due to inclement weather. Santa was able to make the trip with the assistance of Rudolph the Red Nosed Reindeer. The little known behind the scenes efforts of Hermey made it possible for Rudolph to be available for the trip. The abominable snowman (Bumble) had evidently captured Rudolph and friends.  With Rudolph unconscious, Hermey organized a rescue mission with Yukon Cornelius. Upon discovery of the bumble’s real problem, (bad teeth), Hermey with his dental skills, rendered the Bumble a gentle giant. Anesthesia services were provided by Yukon by droping a big rock on the Bumble's head. Rudolph returned unharmed to help guide Santa’s Sleigh! Once again showing the triumph of Dentistry.
With Rudolph unconscious, Hermey organized a rescue mission with Yukon Cornelius. Upon discovery of the bumble’s real problem, (bad teeth), Hermey with his dental skills, rendered the Bumble a gentle giant. Anesthesia services were provided by Yukon by droping a big rock on the Bumble's head. Rudolph returned unharmed to help guide Santa’s Sleigh! Once again showing the triumph of Dentistry.Merry Christmas!
*Followup information on these events may be found here: What Ever Happenned to Hermie the Elf?
Thursday, December 14, 2006
Dakota Fanning on "Braces"

This is a great video of Dakota Fanning last night on the Tonight Show with Jay Leno discussing her "Braces".
*Update December 26, 2006: They have evidently removed this video from Youtube due to copyright issues with NBC. Too bad, as it really shows that even "stars" have the same dental concerns as everyone else. Perhaps, you can check it out on TV in reruns.
Update 2008--I have it here on Youtube:
Monday, December 04, 2006
Self Ligating Orthodontic Brackets
 Recently, self ligating orthodontic brackets have become more popular. They have been around in one form or another for a while, but companies like GAC and 3-M have come out with more refined versions that have some sort of latch to hold the wire in place. The GAC shown here on the left has a clasp (shown in yellow) that moves up to hold the wire in place. We are begining to incorporate some of these into our orthodontic practice. One concern with traditional alastic ligatures or even wire ligatures is the difficulty of proper oral hygiene around the bracket area. The self ligating bracket provides some advantage in this area. The main advantage is that it will take less time to change wires. That means shorter orthodontic appointments for the patient and more efficiency for the doctor and staff. The only problem is that you can't get the cool colors available with alastics.
Recently, self ligating orthodontic brackets have become more popular. They have been around in one form or another for a while, but companies like GAC and 3-M have come out with more refined versions that have some sort of latch to hold the wire in place. The GAC shown here on the left has a clasp (shown in yellow) that moves up to hold the wire in place. We are begining to incorporate some of these into our orthodontic practice. One concern with traditional alastic ligatures or even wire ligatures is the difficulty of proper oral hygiene around the bracket area. The self ligating bracket provides some advantage in this area. The main advantage is that it will take less time to change wires. That means shorter orthodontic appointments for the patient and more efficiency for the doctor and staff. The only problem is that you can't get the cool colors available with alastics.
This one from 3-M has little C clasps on each side.
Tuesday, November 28, 2006
Space Maintainers
If a baby tooth is lost prematurely, you may need a space maintainer to "save" the space. What does that mean? Baby teeth are there for a reason. One key reason is that they save space for the permanent tooth, which will erupt into its position when the baby tooth is lost normally.
If a primary tooth (baby or milk tooth), has to be removed early due to say, an abscess, or is knocked out in some kind of trauma, a space maintainer may be recommended to save the space. If the space is not preserved, the other teeth may drift causing difficult to treat crowding and orthodontic problems. If it is a front tooth then you don't need a space maintainer. However, you can place a Pediatric Partial to replace the teeth for cosmetic reasons.
Now "Spacers" may be in there for a while, but they are not permanent. They are removed when the new tooth (usually a bicuspid) erupts or the abutment teeth get loose.
Kinds of Space Maintainers:
1. Fixed Space Maintainers:

a. Unilateral: Just on one side, usually "replacing" one tooth. Can be a band and loop as you see here, or a crown and loop type (in photo below). This can also be a Distal Shoe type. The distal shoe being one used when the permanent first molar has not yet erupted. Hey, you are usually going to get "silver" in there no matter what kind of spacer it is.

Distal Shoe Type for unerupted 1st molar:


b. Bilateral: These are very useful. They are usually cemented with bands on back teeth on both sides connected by a wire just behind the lower incisors. Usually called a Lingual Arch. This can eliminate the need for two unilateral spacers. They are most useful if there is more than one tooth missing or you are trying to keep the lower incisors from tipping. An altered form can incorporate a looped lingual arch to actually move the lower incisors forward (straighten them a little too) before maintaining them in a better position. A maxillary bilateral spacer may incorporate an acrylic button and is called a Nance space maintainer.


2. Removable: I don't use these too often on children, although sometimes they can be fabricated and used in specific cases. There are like orthodontic retainers, with part of the plastic placed in the empty space to keep things from drifting.
*The Color are Photos from University of Washington web site demo. The X-ray is not.
If a primary tooth (baby or milk tooth), has to be removed early due to say, an abscess, or is knocked out in some kind of trauma, a space maintainer may be recommended to save the space. If the space is not preserved, the other teeth may drift causing difficult to treat crowding and orthodontic problems. If it is a front tooth then you don't need a space maintainer. However, you can place a Pediatric Partial to replace the teeth for cosmetic reasons.
Now "Spacers" may be in there for a while, but they are not permanent. They are removed when the new tooth (usually a bicuspid) erupts or the abutment teeth get loose.
Kinds of Space Maintainers:
1. Fixed Space Maintainers:
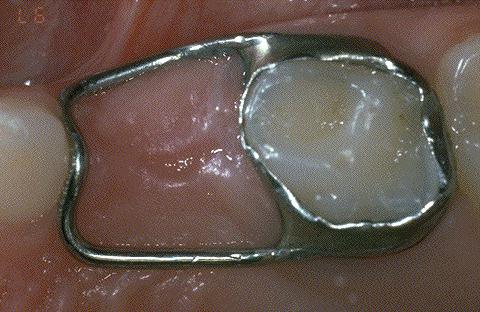
a. Unilateral: Just on one side, usually "replacing" one tooth. Can be a band and loop as you see here, or a crown and loop type (in photo below). This can also be a Distal Shoe type. The distal shoe being one used when the permanent first molar has not yet erupted. Hey, you are usually going to get "silver" in there no matter what kind of spacer it is.

Distal Shoe Type for unerupted 1st molar:


b. Bilateral: These are very useful. They are usually cemented with bands on back teeth on both sides connected by a wire just behind the lower incisors. Usually called a Lingual Arch. This can eliminate the need for two unilateral spacers. They are most useful if there is more than one tooth missing or you are trying to keep the lower incisors from tipping. An altered form can incorporate a looped lingual arch to actually move the lower incisors forward (straighten them a little too) before maintaining them in a better position. A maxillary bilateral spacer may incorporate an acrylic button and is called a Nance space maintainer.


2. Removable: I don't use these too often on children, although sometimes they can be fabricated and used in specific cases. There are like orthodontic retainers, with part of the plastic placed in the empty space to keep things from drifting.
*The Color are Photos from University of Washington web site demo. The X-ray is not.
Wednesday, November 22, 2006
Specialist or Generalist?
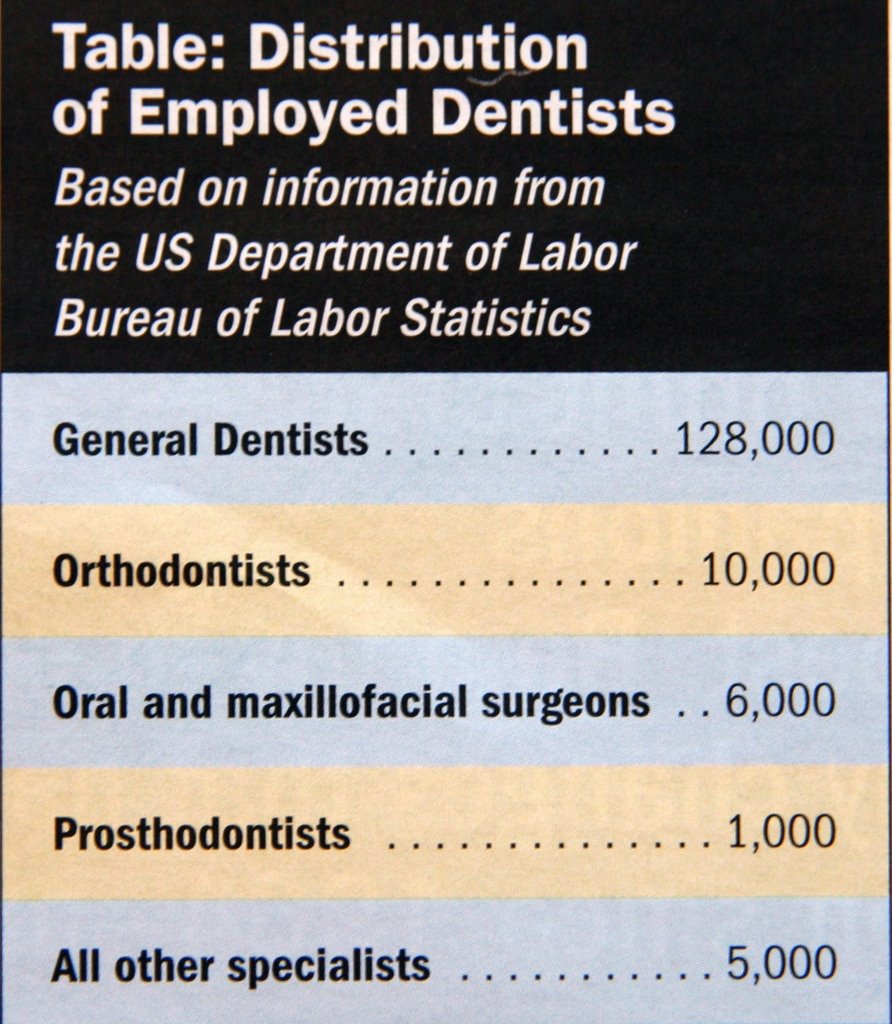
Here is an interesting summary of the distribution of dentists in the United States of America. Most dentists (85%) are General Dentists. About 6% are Orthodontists. If you are a Pediatric Dentist, you are in rare company. Under 3% (about 4000) are blessed to be able to call themselves Pediatric Dentists. See here: The Dental Specialties for more information. More info here too: U.S. government data.
Saturday, November 18, 2006
OrthoCad
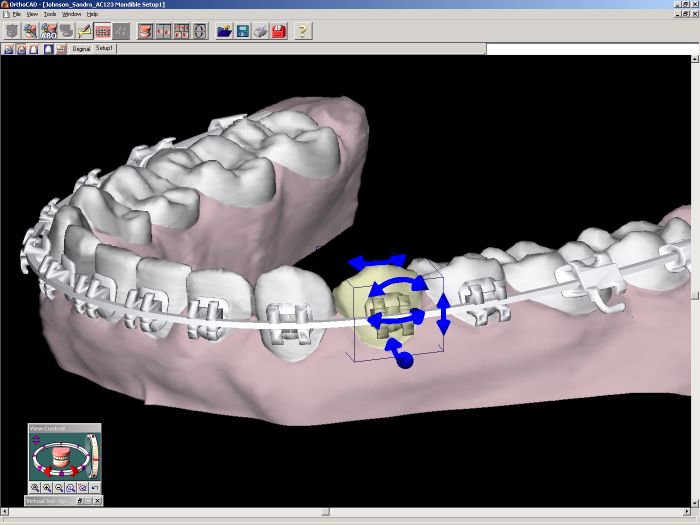 Orthocad is a new service that uses computers to make an indirect bonding set-up for bracket placement. Bracket placement is critical to any case. It is often done by hand placing each bracket. Indirect bonding has been around for several years. You basically make a plaster model from impressions of the patient's mouth. Brackets are placed on the model. A transfer impression is made of the brackets, moving the brackets to the patient in a all at once bonding procedure. The idea is to get the best possible bracket positions and to take less time placing them (which is good for the patient as well).
Orthocad is a new service that uses computers to make an indirect bonding set-up for bracket placement. Bracket placement is critical to any case. It is often done by hand placing each bracket. Indirect bonding has been around for several years. You basically make a plaster model from impressions of the patient's mouth. Brackets are placed on the model. A transfer impression is made of the brackets, moving the brackets to the patient in a all at once bonding procedure. The idea is to get the best possible bracket positions and to take less time placing them (which is good for the patient as well). The new Orthocad system uses impressions, but the models are digitally made and manipulated with computer software. We are just starting to incorporate this in our practice. Here is their web site for more info: OrthoCad
The new Orthocad system uses impressions, but the models are digitally made and manipulated with computer software. We are just starting to incorporate this in our practice. Here is their web site for more info: OrthoCad
Tuesday, November 14, 2006
Can a Tooth get a Cavity Before it Erupts?
 Can a tooth get a cavity before it even erupts into the mouth? Well, in a bacteriological sense, no, but I occassionally see an odd occurance where there is evidently a large radioluscency(dark area) in the coronal (top) part of a unerupted tooth that indicates loss of tooth structure like a cavity would appear. What is it? Technically it cannot be a cavity as that is caused by a bacteriological process. There are no cavity causing bacteria associated with an unerupted tooth. This is due to some kind of abnormal internal resorptive process. The cells in the developing tooth dissolve the tooth from the inside out in a pattern similar to a cavity. When the tooth actually erupts, bacteria go right to the area and starts an actual decay process. So, basically you end up with a really big cavity rapidly. It is necessary to treat these teeth early and agressively. Sometimes they even need a root canal or removal. It's a pretty odd thing to see on an x-ray if you understand the normal decay process. This is not to be confused with developmental defects in the enamel like Enamel Hypoplasia, which is quite common. It is probably more similar to Internal Resorption , which starts in the pulpal tissue rather than the coronal area, but I have to say I don't really know for sure what causes it.
Can a tooth get a cavity before it even erupts into the mouth? Well, in a bacteriological sense, no, but I occassionally see an odd occurance where there is evidently a large radioluscency(dark area) in the coronal (top) part of a unerupted tooth that indicates loss of tooth structure like a cavity would appear. What is it? Technically it cannot be a cavity as that is caused by a bacteriological process. There are no cavity causing bacteria associated with an unerupted tooth. This is due to some kind of abnormal internal resorptive process. The cells in the developing tooth dissolve the tooth from the inside out in a pattern similar to a cavity. When the tooth actually erupts, bacteria go right to the area and starts an actual decay process. So, basically you end up with a really big cavity rapidly. It is necessary to treat these teeth early and agressively. Sometimes they even need a root canal or removal. It's a pretty odd thing to see on an x-ray if you understand the normal decay process. This is not to be confused with developmental defects in the enamel like Enamel Hypoplasia, which is quite common. It is probably more similar to Internal Resorption , which starts in the pulpal tissue rather than the coronal area, but I have to say I don't really know for sure what causes it.
Tuesday, November 07, 2006
Disney "Magic"
 I just got back from a very nice Disney Cruise Line vacation on the Disney Magic, one of Disney's cruise ships. We went for the 7 day cruise. I was quite impressed with the organization of the entire operation. The entire staff (cast memebers as they call themselves), worked constantly to make our vacation a great one. The children were kept entertained and all of us were well fed. I felt a little guilty having so much fun while they worked so hard. I am impressed with their corporate style and management. Their methods might apply to most dental offices, especially pediatric offices. Some of the Disney "service guidelines" includes the following:
I just got back from a very nice Disney Cruise Line vacation on the Disney Magic, one of Disney's cruise ships. We went for the 7 day cruise. I was quite impressed with the organization of the entire operation. The entire staff (cast memebers as they call themselves), worked constantly to make our vacation a great one. The children were kept entertained and all of us were well fed. I felt a little guilty having so much fun while they worked so hard. I am impressed with their corporate style and management. Their methods might apply to most dental offices, especially pediatric offices. Some of the Disney "service guidelines" includes the following:-Make eye contact and smile.
-Greet and welcome every Guest.
-Seek out Guest contact.
-Provide immediate service.
-Display appropriate body language.
-Preserve "Magical" Guest experience.
-Thank each and every Guest.
Most of us would certainly aspire to be that good at patient/parent relations. If we in the dental profession can emulate such service, I think we will be doing our patients a great service.
Thursday, October 19, 2006
Don't Bite Your Numb Lip!
When we do a large filling, remove a tooth, or some other fairly invasive procedure, we "numb" up the area with "novocaine". Well, really more specifically Lidocaine or Mepivicaine . Anyways, the obvious advantage of numbing is there is no pain or discomfort related to the procedure. However, the lip, tooth, gums, and sometimes part of the tongue will be numb for a few hours. Some kids don't quite know how to deal with this numb lip. Unfortunately, some will bite their lip causing it to swell dramatically. They can't feel that they are doing damage.
 Biting a numb lip thankfully does not occur that often. However, I can often spot the kid that is at risk. He is the one fiddling with his lip, sucking it between his teeth, scratching his chin and is otherwise preoccupied with the numb feeling. I always, I mean always, warn the child (and the parent) to not bite on the lip, not to pinch or scratch it either. If they do, it can take a few days for the swelling to go down. You can try an ice pack to limit the swelling in the first few hours. There is sometimes a white/yellow scab inside the lip or cheek. Thankfully, it almost always heals up within a few days. It's best to let your dentist know if you are concerned. Those are the kids to really watch the next time and to avoid numbing unless it's really necessary the next time. If we have a calm child and there is a really small cavity to be filled, there is often no need to numb up the tooth; the kids do quite well.
Biting a numb lip thankfully does not occur that often. However, I can often spot the kid that is at risk. He is the one fiddling with his lip, sucking it between his teeth, scratching his chin and is otherwise preoccupied with the numb feeling. I always, I mean always, warn the child (and the parent) to not bite on the lip, not to pinch or scratch it either. If they do, it can take a few days for the swelling to go down. You can try an ice pack to limit the swelling in the first few hours. There is sometimes a white/yellow scab inside the lip or cheek. Thankfully, it almost always heals up within a few days. It's best to let your dentist know if you are concerned. Those are the kids to really watch the next time and to avoid numbing unless it's really necessary the next time. If we have a calm child and there is a really small cavity to be filled, there is often no need to numb up the tooth; the kids do quite well.
 Biting a numb lip thankfully does not occur that often. However, I can often spot the kid that is at risk. He is the one fiddling with his lip, sucking it between his teeth, scratching his chin and is otherwise preoccupied with the numb feeling. I always, I mean always, warn the child (and the parent) to not bite on the lip, not to pinch or scratch it either. If they do, it can take a few days for the swelling to go down. You can try an ice pack to limit the swelling in the first few hours. There is sometimes a white/yellow scab inside the lip or cheek. Thankfully, it almost always heals up within a few days. It's best to let your dentist know if you are concerned. Those are the kids to really watch the next time and to avoid numbing unless it's really necessary the next time. If we have a calm child and there is a really small cavity to be filled, there is often no need to numb up the tooth; the kids do quite well.
Biting a numb lip thankfully does not occur that often. However, I can often spot the kid that is at risk. He is the one fiddling with his lip, sucking it between his teeth, scratching his chin and is otherwise preoccupied with the numb feeling. I always, I mean always, warn the child (and the parent) to not bite on the lip, not to pinch or scratch it either. If they do, it can take a few days for the swelling to go down. You can try an ice pack to limit the swelling in the first few hours. There is sometimes a white/yellow scab inside the lip or cheek. Thankfully, it almost always heals up within a few days. It's best to let your dentist know if you are concerned. Those are the kids to really watch the next time and to avoid numbing unless it's really necessary the next time. If we have a calm child and there is a really small cavity to be filled, there is often no need to numb up the tooth; the kids do quite well.
Saturday, October 14, 2006
Dr. Clifton O. Dummett, Jr.-A Great Teacher
 Dr. "Cliff" Dummett, was one of the best professors I have had the privilege of coming into contact with in my career. He was at the LSU School of Dentistry Department of Pediatric Dentistry when I was in my residency there. He passed away the other day at age 62 after a long illness. Dr. Dummett had a talent quite lacking in most dental school faculty; he was a good teacher. He always had a smile on his face and could tell you that you screwed up without making you feeling like an idiot. He encouraged you to improve and excel. He and his wife lost their home (and really cool sail boat he once let me pilot) to hurricane Katrina, then moved to Baton Rouge. I send my best wishes to his wife. Thank you Dr. Dummett. I will always remember that smile.
Dr. "Cliff" Dummett, was one of the best professors I have had the privilege of coming into contact with in my career. He was at the LSU School of Dentistry Department of Pediatric Dentistry when I was in my residency there. He passed away the other day at age 62 after a long illness. Dr. Dummett had a talent quite lacking in most dental school faculty; he was a good teacher. He always had a smile on his face and could tell you that you screwed up without making you feeling like an idiot. He encouraged you to improve and excel. He and his wife lost their home (and really cool sail boat he once let me pilot) to hurricane Katrina, then moved to Baton Rouge. I send my best wishes to his wife. Thank you Dr. Dummett. I will always remember that smile.
Friday, October 13, 2006
Please Link Your Blog To This One
If you have enjoyed this blog or otherwise have found it useful or entertaining, please link it to your blog or web site. It's easy to do. You just make a post with a link or create a link in your sidebar with the link code. If you use blogger, go to your template and look at the sidebar links already there. Copy or use the code there and substitute my main URL and Title; very easy
The more links there are to this blog, the more people are likely to find it when using a search engine. Thanks!
The more links there are to this blog, the more people are likely to find it when using a search engine. Thanks!
Wednesday, October 11, 2006
Dental Insurance-Part 2: How it really works
Most people really don't understand their insurance coverage. They usually assume if they pay the premium, they won't have to pay anything. The reality is that insurance is so complicated and is some ways deceptive, that most people don't realize what companies are doing. Deductables, percentage of coverage, delay in payments, downcoding (changing) of procedures to reduce payment, not covering certain procedures at all. All this can set up expectations of complete coverage that cannot be met. Your policy is so complicated you really didn't realize what has transpired. Although he can guess, the dentist cannot definately tell you what your company will pay. Every patient in there has a different policy with different terms. Even then, companies often change their coverage terms. Also, the insurance company will not send you, the patient, the claim check, they send it to the dentist. So generally, you do not pay the whole bill when you have the treatment done like most regular purchases. You may be asked to pay an estimated copay or simply have the dentist file the claim and wait for a bill later. Here is the example similar to the one I mentioned in Part-1. Confusing isn't it:
You go to the dentist and your child has a "cleaning", x-rays, a complete examination. Then he has a white filling and a crown with a pulpotomy with a little laughing gas to relax him. Not a lot of work, but at least you got the problem solved. Your dentist files your insurance. You pay the known deductable. Then, after a few months, you get a bill from the dentist for the amount not covered by the insurance. You are confused. You knew about the deductable, but the rest is pretty much covered, right?
The cleaning, exam and x-rays were covered at, say "100%", and you had a $50 deductable on the remaining treatment with 80% coverage on the amount after that.
What the insurance company will actually do, is downcode the white filling to a "silver" filling (a paperwork trick that pays on a less expensive procedure you didn't actually have done). They reduce the total "fee" on other procedures to their predetermined (ie. made up) "fair" amount, then pay 80% of that, not the original amount. Then, you had forgotten, they only pay 50% of endodontics (the pulpotomy), and they don't even cover the laughing gas at all. Oh, yes, the deductable. It adds up. Your other child (say, from your first marriage), is covered under another plan that has different coverage, so you are confused at the difference in coverage. You get a bill from the dentist. Are you mad? Sure. Where should that anger be targeted? Just remember the dentist hasn't been paid in two or three months, has paid staff to file the claim for you and refile it when the insurance co. "lost" the claim. They tried to estimate the cost for you in the beginning and offered financial arrangements for the remaining amount. They deal with thousands of policies and are doing their best to sort it all out too. What this has done I fear, is breakdown some of the trust in the dentist patient relationship. Not from anything they have done, but from the outside force of the "middleman" of insurance. Some level of confusion and misscommunication could lead to more of an advisary type relationship more common in car dealerships. I hope not.
Insurance companies are in the business of insurance to make money. This is not a bad thing. In most circumstances, their customer is not the patient but employers. What you hopefully get is peace of mind for unexpected expenses. Is it worth it? As I mentioned before, dental services are a statistically predictable non-catastrophic expense. If you have it, well of course use it. Otherwise, each person will have to make up their mind if it is really worth it. I don't want to sound too down on insurance. As I alluded to earlier, some people can benefit from insurance. Some simply cannot afford to pay the entire bill out of pocket if the treatment needs are extensive. I just don't like to see the parent of a patient decline treatment for their child for supposedly financial reasons because dental insurance doesn't cover 100% of the treatment cost. Then, they take a call on their cell phone and drive off in their new Lexus. Priorities.
Know what your insurance policy actually covers, and understand it will be confusing. Remember, the dentist is just as much of a victim of this confusion as the patient. Dentists, remember the patient doesn't always have all the details of their policy that they didn't even pick. Their employer is the one who asked for the cheapest policy. If everyone has some tolerance and understanding, the trust that is the dentist patient relationship can withstand these outside forces.
Dental Insurance-Part 1: A Good Idea?
You go to the dentist and your child has a "cleaning", x-rays, a complete examination. Then he has a white filling and a crown with a pulpotomy with a little laughing gas to relax him. Not a lot of work, but at least you got the problem solved. Your dentist files your insurance. You pay the known deductable. Then, after a few months, you get a bill from the dentist for the amount not covered by the insurance. You are confused. You knew about the deductable, but the rest is pretty much covered, right?
The cleaning, exam and x-rays were covered at, say "100%", and you had a $50 deductable on the remaining treatment with 80% coverage on the amount after that.
What the insurance company will actually do, is downcode the white filling to a "silver" filling (a paperwork trick that pays on a less expensive procedure you didn't actually have done). They reduce the total "fee" on other procedures to their predetermined (ie. made up) "fair" amount, then pay 80% of that, not the original amount. Then, you had forgotten, they only pay 50% of endodontics (the pulpotomy), and they don't even cover the laughing gas at all. Oh, yes, the deductable. It adds up. Your other child (say, from your first marriage), is covered under another plan that has different coverage, so you are confused at the difference in coverage. You get a bill from the dentist. Are you mad? Sure. Where should that anger be targeted? Just remember the dentist hasn't been paid in two or three months, has paid staff to file the claim for you and refile it when the insurance co. "lost" the claim. They tried to estimate the cost for you in the beginning and offered financial arrangements for the remaining amount. They deal with thousands of policies and are doing their best to sort it all out too. What this has done I fear, is breakdown some of the trust in the dentist patient relationship. Not from anything they have done, but from the outside force of the "middleman" of insurance. Some level of confusion and misscommunication could lead to more of an advisary type relationship more common in car dealerships. I hope not.
Insurance companies are in the business of insurance to make money. This is not a bad thing. In most circumstances, their customer is not the patient but employers. What you hopefully get is peace of mind for unexpected expenses. Is it worth it? As I mentioned before, dental services are a statistically predictable non-catastrophic expense. If you have it, well of course use it. Otherwise, each person will have to make up their mind if it is really worth it. I don't want to sound too down on insurance. As I alluded to earlier, some people can benefit from insurance. Some simply cannot afford to pay the entire bill out of pocket if the treatment needs are extensive. I just don't like to see the parent of a patient decline treatment for their child for supposedly financial reasons because dental insurance doesn't cover 100% of the treatment cost. Then, they take a call on their cell phone and drive off in their new Lexus. Priorities.
Know what your insurance policy actually covers, and understand it will be confusing. Remember, the dentist is just as much of a victim of this confusion as the patient. Dentists, remember the patient doesn't always have all the details of their policy that they didn't even pick. Their employer is the one who asked for the cheapest policy. If everyone has some tolerance and understanding, the trust that is the dentist patient relationship can withstand these outside forces.
Dental Insurance-Part 1: A Good Idea?
Dental Insurance-Part 1: A Good Idea?
Dental Insurance has been a good and a bad thing for Dentistry in my opinion. Over the past 15 years, the insurance industry has grown to cover many Americans with dental insurance. This is usually provided through their employers. It does provide some benefit in certain circumstances. Is it a good idea? The comparison should be made to the way it used to be before the large degree of coverage available today. Insurance has traditionally been useful to cover catastrophic unexpected expenses due to things like severe medical conditions, disability, death, fire, tornado damage, etc. Companies are paid a premium per month for the promise of a certain amount of financial coverage if these disasters occur. Good health insurance is a must, and fire coverage for your house is a requirement for your mortgage. It protects you against an unforseen event that could wipe you out financially. Insurance has generally not been used for everyday expenses such as gasoline, groceries, and other non catastrophic expenses. Dentistry is a disease process and is certainly a significant medical condition. It is , however, predictable, and with the exception of cancer and severe trauma (which would be covered under medical insurance anyways), non-catastrophic. In general, why is this a flawed system?
Why would you purchase dental insurance? "I don't, my employer does". Well, you are paying for it, but usually indirectly. Your employer pays the premiums and deducts the cost in the form of a lower salary that you would otherwise receive. The decisions are made by the employer in response to the perceived demand from employees. Coverage is often an "add on" to health insurance. Dental insurance can provide someone who has extensive dental treatment needs with the financial confidence to proceed with treatment when otherwise they could not "afford" it. They would rather have the insurance in lieu of salary. This has benefited many people over time. The insurance, however, becomes the middleman. Sometimes, when a patient has proposed treatment, the response isn't "when can I schedule that", it's "let me see if my insurance covers that". I guess I don't blame them, it's just way different than before.
If I told you I was selling gasoline insurance, would you buy it? I will ask for premium payment every month. In exchange, you send me your receipts from the gas station. I will then send you a check for these "claims" you have made. Would you buy that? I would advise you to say no to this deal. Why? With the money you are paying every month you could just pay for the gas anyways. Your gasoline purchases are predictable and non-catastrophic.
Is that a good deal? No, this is silly.
I know this is exagerated, but you see the point. By the way, be reminded if your employer "pays the premium", just remember that check went to the insurance company instead of your salary.
Dentistry, more specifically dental costs are more predictable and less expensive than medical emergencies. After looking at the real costs of dentistry and the actual premiums, deductables, etc. My determination is that, for most people, it is not worth it. If your company provides the insurance, well of course use it, but understand what it actually covers. It is only really worth it however, if you know you have lots of dentistry that is going to be required over a specific period of time, like massive crowns, bridges, surgeries, etc. It may be worth it until you were stabilized into routine care. So, unless you fall into that catagory, save your money and use that to pay the dentist instead of the insurance company. I'll have more posts on dental insurance and dentistry in the near future.
Dental Insurance-Part 2: How it Really Works
ADA Site: Dental Insurance FAQ
Another great link:
How Dental Insurance Works
Why would you purchase dental insurance? "I don't, my employer does". Well, you are paying for it, but usually indirectly. Your employer pays the premiums and deducts the cost in the form of a lower salary that you would otherwise receive. The decisions are made by the employer in response to the perceived demand from employees. Coverage is often an "add on" to health insurance. Dental insurance can provide someone who has extensive dental treatment needs with the financial confidence to proceed with treatment when otherwise they could not "afford" it. They would rather have the insurance in lieu of salary. This has benefited many people over time. The insurance, however, becomes the middleman. Sometimes, when a patient has proposed treatment, the response isn't "when can I schedule that", it's "let me see if my insurance covers that". I guess I don't blame them, it's just way different than before.
If I told you I was selling gasoline insurance, would you buy it? I will ask for premium payment every month. In exchange, you send me your receipts from the gas station. I will then send you a check for these "claims" you have made. Would you buy that? I would advise you to say no to this deal. Why? With the money you are paying every month you could just pay for the gas anyways. Your gasoline purchases are predictable and non-catastrophic.
Is that a good deal? No, this is silly.
I know this is exagerated, but you see the point. By the way, be reminded if your employer "pays the premium", just remember that check went to the insurance company instead of your salary.
Dentistry, more specifically dental costs are more predictable and less expensive than medical emergencies. After looking at the real costs of dentistry and the actual premiums, deductables, etc. My determination is that, for most people, it is not worth it. If your company provides the insurance, well of course use it, but understand what it actually covers. It is only really worth it however, if you know you have lots of dentistry that is going to be required over a specific period of time, like massive crowns, bridges, surgeries, etc. It may be worth it until you were stabilized into routine care. So, unless you fall into that catagory, save your money and use that to pay the dentist instead of the insurance company. I'll have more posts on dental insurance and dentistry in the near future.
Dental Insurance-Part 2: How it Really Works
ADA Site: Dental Insurance FAQ
Another great link:
How Dental Insurance Works
Sunday, October 01, 2006
Sedation Tragedy
Her name was Diamond. The little 5 year old who died the other day. She had lapsed into a coma after receiving sedative medications for treatment in a Chicago dental office. We don't yet know what happened. Reports are that she received medications via three different routes including IV. We do not know if the child had any predisposing medical conditions. It appears she went into a deep sedative state and lost her respiratory function; she stopped breathing on her own. We don't yet know what occurred.
This is a very rare event, in fact:
 No child has ever died as the result of any dental sedation that has been done in accordance with the Academy of Pediatric Dentistry's guidelines. I know in our state (Alabama) you can only intentionally put the child in a state of conscious sedation (not deep sedation), otherwise you have to follow different protocols, equipment and licensure requirements, like a hospital. I personally have never know of any severe complications in our area.
No child has ever died as the result of any dental sedation that has been done in accordance with the Academy of Pediatric Dentistry's guidelines. I know in our state (Alabama) you can only intentionally put the child in a state of conscious sedation (not deep sedation), otherwise you have to follow different protocols, equipment and licensure requirements, like a hospital. I personally have never know of any severe complications in our area.
Most kids do quite well without any kind of extra medication to accomplish treatment. However, sometimes medications are needed to help kids to be comfortable and cooperate to accomplish treatment. Sometimes it is even necessary to do treatment under General Anesthesia in the Hospital. Many times, however, the hospital is not an option due to lack of insurance coverage, limited treatment needs, or parental preference. The option of in office conscious sedation has been a good option to help kids and parents. After extensive training and experience, I use this valuable method of providing treatment nearly every day and am very confident in the use of medications to relieve discomfort, reduce anxiety and provide a safe environment through concious sedation. Every time a parent puts their child in my care, I pray I have the knowledge, skill, and compassion to keep that child safe. Things can be unpredictable. Bad things can happen to anyone, but knowing that, like the Boy Scout motto says: be prepared. God willing, this will never happen again no matter what the reason.
More information here: Sedation in Pediatric Dentistry
Update August 17, 2007: I just saw a news piece on Fox News. Now I like Fox News, but the "news report" was a little overboard. Although the story alluded to the incident with Diamond, most of the story really had little to do with that particular incident. One of the physicians speculated that Diamond had a pre-existing medical condition (which is not improbable). However, the headline of the story was "is laughing gas safe?". What? Patients are awake during nitrous oxide administration. The doctors on the program did give a rational answer that it is safe. In fact, it likely had nothing to do with this unfortunate incident. These very rare problems tend to arise with over-dosage of much stronger medications and the interaction between them combined with pre-existing unknown medical conditions and improper monitoring of the patient. Even local anesthetic can interact with other medicines to create an adverse reaction. I think this news piece will just create unnecessary anxiety in parents that is not based on any scientific or rational information.
Update December 2007: In "Pediatric Dentistry Today" Sept. 2007, Volume XLIII, Number 5, it was reported the child had very large dosages of multiple oral and IV medications. My conclusion is that it was primarily an overdose situation that was not monitored nor handled correctly all along the way.
This is a very rare event, in fact:
 No child has ever died as the result of any dental sedation that has been done in accordance with the Academy of Pediatric Dentistry's guidelines. I know in our state (Alabama) you can only intentionally put the child in a state of conscious sedation (not deep sedation), otherwise you have to follow different protocols, equipment and licensure requirements, like a hospital. I personally have never know of any severe complications in our area.
No child has ever died as the result of any dental sedation that has been done in accordance with the Academy of Pediatric Dentistry's guidelines. I know in our state (Alabama) you can only intentionally put the child in a state of conscious sedation (not deep sedation), otherwise you have to follow different protocols, equipment and licensure requirements, like a hospital. I personally have never know of any severe complications in our area.Most kids do quite well without any kind of extra medication to accomplish treatment. However, sometimes medications are needed to help kids to be comfortable and cooperate to accomplish treatment. Sometimes it is even necessary to do treatment under General Anesthesia in the Hospital. Many times, however, the hospital is not an option due to lack of insurance coverage, limited treatment needs, or parental preference. The option of in office conscious sedation has been a good option to help kids and parents. After extensive training and experience, I use this valuable method of providing treatment nearly every day and am very confident in the use of medications to relieve discomfort, reduce anxiety and provide a safe environment through concious sedation. Every time a parent puts their child in my care, I pray I have the knowledge, skill, and compassion to keep that child safe. Things can be unpredictable. Bad things can happen to anyone, but knowing that, like the Boy Scout motto says: be prepared. God willing, this will never happen again no matter what the reason.
More information here: Sedation in Pediatric Dentistry
Update August 17, 2007: I just saw a news piece on Fox News. Now I like Fox News, but the "news report" was a little overboard. Although the story alluded to the incident with Diamond, most of the story really had little to do with that particular incident. One of the physicians speculated that Diamond had a pre-existing medical condition (which is not improbable). However, the headline of the story was "is laughing gas safe?". What? Patients are awake during nitrous oxide administration. The doctors on the program did give a rational answer that it is safe. In fact, it likely had nothing to do with this unfortunate incident. These very rare problems tend to arise with over-dosage of much stronger medications and the interaction between them combined with pre-existing unknown medical conditions and improper monitoring of the patient. Even local anesthetic can interact with other medicines to create an adverse reaction. I think this news piece will just create unnecessary anxiety in parents that is not based on any scientific or rational information.
Update December 2007: In "Pediatric Dentistry Today" Sept. 2007, Volume XLIII, Number 5, it was reported the child had very large dosages of multiple oral and IV medications. My conclusion is that it was primarily an overdose situation that was not monitored nor handled correctly all along the way.
Friday, September 29, 2006
They Are Just Baby Teeth, Why Fix Them?
They are just baby teeth, why fix them?
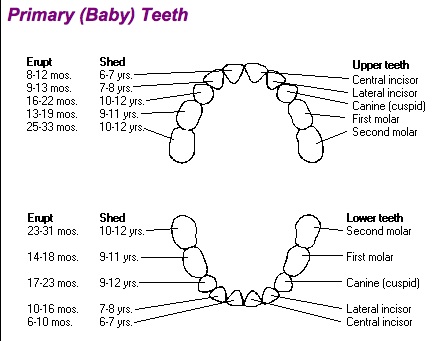
Most babies get their first tooth around 6 or 7 months of age; usually the bottom front two incisors. Some kids are a little slower erupting the first tooth causing parental worry. It can be even around 12 months for the first one to poke through. Additional baby teeth will continue to come in till almost three years of age. There really is a lot of variability on the sequence. Don’t feel bad if your child does not get his teeth just like your neighbor’s baby or even his own twin sister. This is important: look at the chart below and you will see that some baby teeth START falling out around 5-6 years old (again give or take a little), but the back molars do not fall out till around 12 years of age!
If your child develops a cavity in a baby tooth the decay will slowly (and sometimes rapidly) get bigger and deeper. If the tooth is really close to falling out, we have the option of just leaving it alone. If it looks like it may be a while till it would normally fall out, we need to do something. Otherwise you are in for ugly teeth, toothaches, infection and more extensive dental work.
A small cavity can be filled with a white filling, a medium cavity can be filled, but a deep or large cavity may need a crown to cover the whole tooth. If the tooth is in the back, the crown may be silver in color. It may even need a Pulpotomy or “nerve treatment”. So, get it fixed early when it is small (and less expensive)!
Remember baby teeth are there for a reason. They give the child something to chew with and (importantly) they often save space for the permanent teeth. Why don't you just pull it? Well, sometimes that is the best option, but if a back baby tooth is lost too early, without followup treatment, additional crowding problems that are often more difficult to correct will occur. So you usually will need additional work like a Space Maintainer. That's one reason why it's often easier to fix a baby tooth than just remove it.
Here is an ADA eruption chart for general reference:
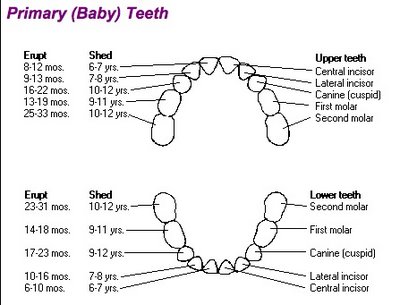
Most babies get their first tooth around 6 or 7 months of age; usually the bottom front two incisors. Some kids are a little slower erupting the first tooth causing parental worry. It can be even around 12 months for the first one to poke through. Additional baby teeth will continue to come in till almost three years of age. There really is a lot of variability on the sequence. Don’t feel bad if your child does not get his teeth just like your neighbor’s baby or even his own twin sister. This is important: look at the chart below and you will see that some baby teeth START falling out around 5-6 years old (again give or take a little), but the back molars do not fall out till around 12 years of age!
If your child develops a cavity in a baby tooth the decay will slowly (and sometimes rapidly) get bigger and deeper. If the tooth is really close to falling out, we have the option of just leaving it alone. If it looks like it may be a while till it would normally fall out, we need to do something. Otherwise you are in for ugly teeth, toothaches, infection and more extensive dental work.
A small cavity can be filled with a white filling, a medium cavity can be filled, but a deep or large cavity may need a crown to cover the whole tooth. If the tooth is in the back, the crown may be silver in color. It may even need a Pulpotomy or “nerve treatment”. So, get it fixed early when it is small (and less expensive)!
Remember baby teeth are there for a reason. They give the child something to chew with and (importantly) they often save space for the permanent teeth. Why don't you just pull it? Well, sometimes that is the best option, but if a back baby tooth is lost too early, without followup treatment, additional crowding problems that are often more difficult to correct will occur. So you usually will need additional work like a Space Maintainer. That's one reason why it's often easier to fix a baby tooth than just remove it.
Here is an ADA eruption chart for general reference:
Monday, September 25, 2006
Female Pediatric Dentists
The most recent volume of the Journal of "Pediatric Dentistry" Vol. 28, No. 5, September/October 2006 had a study of pediatric dentistry program applicants and pediatric dentistry residents. It found that the quality of applicants is increasing and that the proportion of female pediatric dental residents is rising as well. In fact, of pediatric dentistry applicants (those that have graduated dental school and are applying to a residency), almost 60% are female!
Wednesday, September 20, 2006
Torn Maxillary Frenum in a Child
If a young child has hit his mouth, and there is lots of blood especially on his upper teeth lip area, look and see if it might just be a torn maxillary frenum. That's the little piece of tissue that connects the upper lip to the gum between the two front teeth. If it was tight and gets hit and stretched too much it will tear. It bleeds a lot at first, but will likely be fine after 20 minutes or so. Usually no stitches are necessary. In fact there may be no treatment needed at all. This is a very common injury in preschoolers.
More info on dental accidents here:
Dental Accidents (with links to related posts)
More info on dental accidents here:
Dental Accidents (with links to related posts)
Wednesday, September 13, 2006
Just Got an e-mail-Bad Decay on a Two Year Old's Teeth
I just received an e-mail from a concerned parent regarding extensive decay on a two year old. This is otherwise known as baby bottle tooth decay. Here is some of my reply:
1. Decay is caused by bacteria. Some kids pick it up and some don’t. We really don’t understand all the mechanisms. So, for one thing don’t blame yourself for the decay.
2. Yes, sometimes a bottle or sippy-cup (at night) can speed up the process, but most kids need milk, etc. during the day to get enough nutrition to grow healthy. The AAPD recommends getting them off the nighttime bottle (juice etc.) around one year of age. Of course that sometimes can be easier said than done. My own daughter loved the bottle, so I switched to just water. She wasn’t so keen on the water I must say, but it worked.
3. Don’t feel like you are the only one with this problem. I see it every day!
4. Now on cavities. How bad it is cannot be determined easily be appearance. I have to get in there and look around and feel of the area with little tools. If the decay “looks really bad”, like very black in color, that might actually be not so bad. I worry more about the decay that looks more light brown or yellow as it is growing so rapidly it has not yet picked up the stain the slower progressing “black’ decay has. In fact the brown or yellow decay may be much deeper than it looks on the surface.
5. Once decay starts, it usually does not stop. It only gets deeper and spreads.
6. A small cavity can be restored with a small White Filling, but remember the same predisposing factors that started the cavity in the first place are still there. So you can get recurrent decay later on. A medium cavity can be filled with a medium filling. A widespread cavity often needs a crown even if it’s not deep. A deep cavity may go very close to the pulp (nerve) or even infect the pulp. If that happens you are looking at some kind of pulpal therapy (like a Pulpotomy) or removal of the tooth if it’s actually abscessed. If the tooth has so much decay (and it can be deceptive how much decay there is in there) that you really can’t even hang a crown on there, I will recommend removal.
So where does that leave us. We as parents want the teeth “fixed”*, sometimes at all costs. That can be done in many cases. Sometimes it is better to remove the teeth to avoid the future complications of a “restored” tooth. If a back tooth is removed early, we usually recommend a space maintainer. If it is one of those front teeth on top, I know you really want to fix them, but if we have to remove them there is no need for a space maintainer. Speech will develop normally and only us parents care about the appearance. It also reduces the risk to the permanent teeth by having no “sick” tooth near it. Sometimes some kind of fake teeth (a Partial) can be placed for looks only. Not my first choice, but we do make tem from time to time. Usually that’s on a child that’s old enough to cooperate and has all their teeth (three or four years old). Remember, once he starts school, some kids are already loosing some teeth and it’s more normal. However, the upper front teeth don’t usually come in till age seven.
*They Are Just baby Teeth, Why Fix Them?
1. Decay is caused by bacteria. Some kids pick it up and some don’t. We really don’t understand all the mechanisms. So, for one thing don’t blame yourself for the decay.
2. Yes, sometimes a bottle or sippy-cup (at night) can speed up the process, but most kids need milk, etc. during the day to get enough nutrition to grow healthy. The AAPD recommends getting them off the nighttime bottle (juice etc.) around one year of age. Of course that sometimes can be easier said than done. My own daughter loved the bottle, so I switched to just water. She wasn’t so keen on the water I must say, but it worked.
3. Don’t feel like you are the only one with this problem. I see it every day!
4. Now on cavities. How bad it is cannot be determined easily be appearance. I have to get in there and look around and feel of the area with little tools. If the decay “looks really bad”, like very black in color, that might actually be not so bad. I worry more about the decay that looks more light brown or yellow as it is growing so rapidly it has not yet picked up the stain the slower progressing “black’ decay has. In fact the brown or yellow decay may be much deeper than it looks on the surface.
5. Once decay starts, it usually does not stop. It only gets deeper and spreads.
6. A small cavity can be restored with a small White Filling, but remember the same predisposing factors that started the cavity in the first place are still there. So you can get recurrent decay later on. A medium cavity can be filled with a medium filling. A widespread cavity often needs a crown even if it’s not deep. A deep cavity may go very close to the pulp (nerve) or even infect the pulp. If that happens you are looking at some kind of pulpal therapy (like a Pulpotomy) or removal of the tooth if it’s actually abscessed. If the tooth has so much decay (and it can be deceptive how much decay there is in there) that you really can’t even hang a crown on there, I will recommend removal.
So where does that leave us. We as parents want the teeth “fixed”*, sometimes at all costs. That can be done in many cases. Sometimes it is better to remove the teeth to avoid the future complications of a “restored” tooth. If a back tooth is removed early, we usually recommend a space maintainer. If it is one of those front teeth on top, I know you really want to fix them, but if we have to remove them there is no need for a space maintainer. Speech will develop normally and only us parents care about the appearance. It also reduces the risk to the permanent teeth by having no “sick” tooth near it. Sometimes some kind of fake teeth (a Partial) can be placed for looks only. Not my first choice, but we do make tem from time to time. Usually that’s on a child that’s old enough to cooperate and has all their teeth (three or four years old). Remember, once he starts school, some kids are already loosing some teeth and it’s more normal. However, the upper front teeth don’t usually come in till age seven.
*They Are Just baby Teeth, Why Fix Them?
Tuesday, September 12, 2006
All My Posts Are Linked on the Sidebar
Well, it has been about a year since I started this blog. The main page has gotten pretty large because I was afraid the really good posts from the beginning would be lost in the Archives and no one will see them. I finally figured out how to add links to all the posts in the sidebar of every page. So, there will be a link to all the posts I have ever made right there. Just click on the subject in which you are interested. The main page will not display all the posts so it will be a more manageable size.
I hope everyone will continue to find the links they need right over there in the sidebar>>>>>>
I hope everyone will continue to find the links they need right over there in the sidebar>>>>>>
What is a Pulpotomy?
A pulpotomy is when the inflamed pulp chamber, usually on a baby molar, is removed, the area is sterilized, and the chamber is sealed. It is sometimes called a baby tooth root canal, but it's not really a root canal and it can be done is some cases in permanent teeth. It is a very common procedure in children and has a reasonably good prognosis of success. It's also fairly easy to do in conjunction with associated procedures.
 When a cavity gets really deep, close to the pulp of a tooth or even into the pulp, the pulpal tissue becomes irritated and inflamed. This is usually the "tooth ache" you feel. If the inflammation and infection continues without treatment, the tooth will likely eventually abscess. In baby molars, a pulpotomy is used in the process of trying to save and restore the tooth. First, the decay is removed, and then the pulp chamber (the top part, not the root canals) is removed usually with a high-speed bur or spoon excavator. A small cotton ball damp with formocresol is placed to "mummify" the pulp stumps and to sterilize the area. After a couple of minutes, the cotton ball is removed and the opening is sealed usually with a Zinc Oxide and Eugenol material like IRM. IRM is a putty like material that hardens up after a few minutes. After a pulpotomy on a baby molar, it is usually necessary to place a stainless steel crown to restore the tooth. The most common method to treat pulpotomized teeth is formocresol. Other methods include Ferric Oxide, MTA, electrosurgery and even lasers.
When a cavity gets really deep, close to the pulp of a tooth or even into the pulp, the pulpal tissue becomes irritated and inflamed. This is usually the "tooth ache" you feel. If the inflammation and infection continues without treatment, the tooth will likely eventually abscess. In baby molars, a pulpotomy is used in the process of trying to save and restore the tooth. First, the decay is removed, and then the pulp chamber (the top part, not the root canals) is removed usually with a high-speed bur or spoon excavator. A small cotton ball damp with formocresol is placed to "mummify" the pulp stumps and to sterilize the area. After a couple of minutes, the cotton ball is removed and the opening is sealed usually with a Zinc Oxide and Eugenol material like IRM. IRM is a putty like material that hardens up after a few minutes. After a pulpotomy on a baby molar, it is usually necessary to place a stainless steel crown to restore the tooth. The most common method to treat pulpotomized teeth is formocresol. Other methods include Ferric Oxide, MTA, electrosurgery and even lasers.
 Pulpotomies have reasonably good prognosis. It may buy some time, but cannot save an already abscessed tooth. It is often surprising to me how a seemingly small area of decay can be deep enough to reach the pulp. This is often due to the varied antomy of baby teeth and the rapid progression of decay. Although a very reliable procedure, rarely, a tooth with a pulpotomy will have complications and need to be extracted. This is usually due to the remaining pulp tissue in the root canals giving some kind of trouble.
Pulpotomies have reasonably good prognosis. It may buy some time, but cannot save an already abscessed tooth. It is often surprising to me how a seemingly small area of decay can be deep enough to reach the pulp. This is often due to the varied antomy of baby teeth and the rapid progression of decay. Although a very reliable procedure, rarely, a tooth with a pulpotomy will have complications and need to be extracted. This is usually due to the remaining pulp tissue in the root canals giving some kind of trouble.
Bottom line: a pulpotomy is a really good and reliable way to save a badly decayed baby tooth.
More info on: Pulpotomy
 When a cavity gets really deep, close to the pulp of a tooth or even into the pulp, the pulpal tissue becomes irritated and inflamed. This is usually the "tooth ache" you feel. If the inflammation and infection continues without treatment, the tooth will likely eventually abscess. In baby molars, a pulpotomy is used in the process of trying to save and restore the tooth. First, the decay is removed, and then the pulp chamber (the top part, not the root canals) is removed usually with a high-speed bur or spoon excavator. A small cotton ball damp with formocresol is placed to "mummify" the pulp stumps and to sterilize the area. After a couple of minutes, the cotton ball is removed and the opening is sealed usually with a Zinc Oxide and Eugenol material like IRM. IRM is a putty like material that hardens up after a few minutes. After a pulpotomy on a baby molar, it is usually necessary to place a stainless steel crown to restore the tooth. The most common method to treat pulpotomized teeth is formocresol. Other methods include Ferric Oxide, MTA, electrosurgery and even lasers.
When a cavity gets really deep, close to the pulp of a tooth or even into the pulp, the pulpal tissue becomes irritated and inflamed. This is usually the "tooth ache" you feel. If the inflammation and infection continues without treatment, the tooth will likely eventually abscess. In baby molars, a pulpotomy is used in the process of trying to save and restore the tooth. First, the decay is removed, and then the pulp chamber (the top part, not the root canals) is removed usually with a high-speed bur or spoon excavator. A small cotton ball damp with formocresol is placed to "mummify" the pulp stumps and to sterilize the area. After a couple of minutes, the cotton ball is removed and the opening is sealed usually with a Zinc Oxide and Eugenol material like IRM. IRM is a putty like material that hardens up after a few minutes. After a pulpotomy on a baby molar, it is usually necessary to place a stainless steel crown to restore the tooth. The most common method to treat pulpotomized teeth is formocresol. Other methods include Ferric Oxide, MTA, electrosurgery and even lasers. Pulpotomies have reasonably good prognosis. It may buy some time, but cannot save an already abscessed tooth. It is often surprising to me how a seemingly small area of decay can be deep enough to reach the pulp. This is often due to the varied antomy of baby teeth and the rapid progression of decay. Although a very reliable procedure, rarely, a tooth with a pulpotomy will have complications and need to be extracted. This is usually due to the remaining pulp tissue in the root canals giving some kind of trouble.
Pulpotomies have reasonably good prognosis. It may buy some time, but cannot save an already abscessed tooth. It is often surprising to me how a seemingly small area of decay can be deep enough to reach the pulp. This is often due to the varied antomy of baby teeth and the rapid progression of decay. Although a very reliable procedure, rarely, a tooth with a pulpotomy will have complications and need to be extracted. This is usually due to the remaining pulp tissue in the root canals giving some kind of trouble.Bottom line: a pulpotomy is a really good and reliable way to save a badly decayed baby tooth.
More info on: Pulpotomy
Wednesday, August 30, 2006
DMD or DDS, What's The Difference?
DMD or DDS, What's The Difference? These are the doctoral degrees awarded upon completion of dental school in the United States. What's the difference? Basically there is no real difference. Schools across the country award either the DDS (Doctor of Dental Surgery) or the DMD (Doctor of Dental Medicine). Several years ago there was a movement in the academic community to increase the amount of medical training in dental school and make it more similar to the MD degree in medicine. Some school's adopted this new DMD program with additional medical training. Well, as the years passed, all programs pretty much have developed the same curriculum regardless of the degree awarded. So, there is no real difference.
Question: Is a DDS an Oral Surgeon? No. Oral Surgery is a Specialty of Dentistry requiring additional years of training.
I have a DMD from the University of Alabama. Other schools awarding the DMD are Harvard University, University of Connecticut, Medical College of Georgia, and several more.
Question: Is a DDS an Oral Surgeon? No. Oral Surgery is a Specialty of Dentistry requiring additional years of training.
I have a DMD from the University of Alabama. Other schools awarding the DMD are Harvard University, University of Connecticut, Medical College of Georgia, and several more.
Huntsville Office Slide Show
Here is a cute little slide show video of our Huntsville office:

Watch the video
We are quite proud of this new facility. We have a NASA space theme. Both our regular pediatric patients and our orthodontic patients are seen here. There is an indoor playground and video games to occcupy the children during their visit. Often the parents can't get the kids to leave when it's time to go! You'll see a lot of these open bay type rooms in Pediatric and Orthodontic offices. There are private treatment rooms as well. We also have a great office in Madison, Alabama as well!
Although we really are proud of our facility, we like to think it's the staff and doctors that make it a fun and special place.
We are quite proud of this new facility. We have a NASA space theme. Both our regular pediatric patients and our orthodontic patients are seen here. There is an indoor playground and video games to occcupy the children during their visit. Often the parents can't get the kids to leave when it's time to go! You'll see a lot of these open bay type rooms in Pediatric and Orthodontic offices. There are private treatment rooms as well. We also have a great office in Madison, Alabama as well!
Although we really are proud of our facility, we like to think it's the staff and doctors that make it a fun and special place.
Tuesday, August 29, 2006
Quality of Life, Huntsville #1
Yes, Huntsville was voted the Number One Military Community of Excellence in the nation. The rating was by Expansion Management Magazine. There are almost 15,ooo active duty military living here in addition to the very large civilian contingent. We at APDA have many children of these service members as our patients. Huntsville, Madison and the whole area have historically been a military friendly place. The U.S. Army has a large presence here in the form of the Army Missile Command and Research facilities. In fact Werner Von Braun's German Rocket team started their program here with the army here after the war. In fact Werner Von Braun used to live just up the street from me when I was a child. The NASA and Army installations here are one reason for the BRAC commission's recommendation to move many people here over the next few years. The local school systems are anticipating 9000 new children over the next few years. We at APDA are in the process of preparing our facilities for that influx of new patients. I am sure many of these families are probably anxious about the move, but I encourage them to take a good long look, as this is one of the best places to live in the USA!
In an earlier ranking in another magazine, Huntsville ranked #2 in the country in the ability of it's residents to increase their net income, that is high salaries and low cost of living. Opportunity doesn't get much better than that. The rest is up to us.
If you are thinkng of moving here, give us a call at APDA for your child's dental needs.
More here on BRAC and the Huntsville area: BRAC: Moving to Huntsville and Madison
In an earlier ranking in another magazine, Huntsville ranked #2 in the country in the ability of it's residents to increase their net income, that is high salaries and low cost of living. Opportunity doesn't get much better than that. The rest is up to us.
If you are thinkng of moving here, give us a call at APDA for your child's dental needs.
More here on BRAC and the Huntsville area: BRAC: Moving to Huntsville and Madison
Friday, August 25, 2006
Top Ten Posts
 Here is a list of the top ten posts over the last year here at Pediatric Dentistry. Yes, I've been doing this for over a year now. The site meter tells me things like what search words are used when using, say msn or google, to find the answer to a question. It seems that certain topics come up again and again. Some people ask how to become a dentist or what do we actually do. Most people seem to want an answer to a specific question or concern. Here is the countdown top ten list with links to popular and informative posts on this blog from this last year:
Here is a list of the top ten posts over the last year here at Pediatric Dentistry. Yes, I've been doing this for over a year now. The site meter tells me things like what search words are used when using, say msn or google, to find the answer to a question. It seems that certain topics come up again and again. Some people ask how to become a dentist or what do we actually do. Most people seem to want an answer to a specific question or concern. Here is the countdown top ten list with links to popular and informative posts on this blog from this last year:10. Orthodontic Fashion Different color braces: this also includes traditional silver braces, gold braces, and clear or invisible braces.
9. The Dental Specialties A summary of the dental specialties with commentary.
8. Aspiring Dentist Saves Christmas! A holiday favorite!
7. Children's Dentistry An overview of what we do More about what we do an a daily basis.
6. How do you Become a Pediatric Dentist or Orthodontist? Basics of what is required.
5. Posterior Crossbite Also about all kinds of crossbites. Very common condition often needing correction. I get lots of requests about this topic I think because it is so common and dentists are recommending needed correction.
4. When is the Best Time to Start Braces? A question often asked, with more than one answer.
3. Fractured Teeth, Knocked out Teeth, and other Pediatric Dental Accidents Basics of pediatric dental trauma.
2. Permanent Tooth Coming in Behind Baby Teeth A very common occurence. You know, baby teeth not falling out in time.
--and the #1 Post on Pediatric dentistry this past year:
1. My Child's Tooth is Turning Dark! I know you're wondering how that has happened and what to do about it.
If you want more, go back to the home page or click here:Pediatric Dentistry
Saturday, August 19, 2006
Tongue Tied
Everyone has this little connection from the floor of the mouth to the underside of the tongue. This is called a lingual frenum. Sometimes it is quite thick and tight, or it may have a connection point close to the the tip of the tongue. If it is too tight or too thick it may interfere with proper tongue movement or speech development. This is called being Tongue Tied. (You can see why they call it that).
Treatment: If the tongue moves pretty well and speech is developing normally, no treatment is indicated. However, sometimes we will recommend surgically clipping the frenum to allow more natural movement, especially if it is really tight or in some other way interfering with normal movement. Now just clipping the frenum will not necessarily correct a speech problem. However, a tongue that is free to move properly will at least reduce one complicating factor. Infants may have a frenum that concerns a parent who is having nursing problems. Most of the time a frenum is not the problem in these cases.
I usually wait till a child is old enough to cooperate a little in the dental office, usually around four years of age. Then it is quite easy using an electrosurge (bovie type) instrument that easily cuts the area with little or no blood involved. The kids do quite well for this. Usually no sutures are needed, although in more extensive cases they may be needed. If I think the case is more severe I will refer to an oral surgeon who can do a more extensive procedures utilizing some sort of general anesthesia. Again, most children don't need a frenum clipped. Each case should be evaluated on an individual basis. This one is pretty tight with a high attachment:

To return to the home page for more info click here: Pediatric Dentistry
Treatment: If the tongue moves pretty well and speech is developing normally, no treatment is indicated. However, sometimes we will recommend surgically clipping the frenum to allow more natural movement, especially if it is really tight or in some other way interfering with normal movement. Now just clipping the frenum will not necessarily correct a speech problem. However, a tongue that is free to move properly will at least reduce one complicating factor. Infants may have a frenum that concerns a parent who is having nursing problems. Most of the time a frenum is not the problem in these cases.
I usually wait till a child is old enough to cooperate a little in the dental office, usually around four years of age. Then it is quite easy using an electrosurge (bovie type) instrument that easily cuts the area with little or no blood involved. The kids do quite well for this. Usually no sutures are needed, although in more extensive cases they may be needed. If I think the case is more severe I will refer to an oral surgeon who can do a more extensive procedures utilizing some sort of general anesthesia. Again, most children don't need a frenum clipped. Each case should be evaluated on an individual basis. This one is pretty tight with a high attachment:

To return to the home page for more info click here: Pediatric Dentistry
Friday, August 18, 2006
Dental Lasers
 Ok, I'll tell you right now, I'm not an expert on dental lasers, but I have seen where the technology is. My father is a physicist, so I should be able to tackle lasers. The dental lasers currently available are quite useful at soft tissue surgery, that is things like gingival contouring. They can be used to treat apthous ulcers and to remove minor lesions like fibromas. Other dental lasers can be used to do some hard tissue surgery (teeth). That is, they can do much of what the dental handpiece (drill) does now. However, they do not totally replace the handpiece and they cannot be used, right now anyways, to prepare crowns, or remove alloy fillings. They do not totally replace dental handpieces.
Ok, I'll tell you right now, I'm not an expert on dental lasers, but I have seen where the technology is. My father is a physicist, so I should be able to tackle lasers. The dental lasers currently available are quite useful at soft tissue surgery, that is things like gingival contouring. They can be used to treat apthous ulcers and to remove minor lesions like fibromas. Other dental lasers can be used to do some hard tissue surgery (teeth). That is, they can do much of what the dental handpiece (drill) does now. However, they do not totally replace the handpiece and they cannot be used, right now anyways, to prepare crowns, or remove alloy fillings. They do not totally replace dental handpieces. How they work is to heat up any water in the area that's zapped till basically it explodes in a little puff. It can be quite precise. Of course, with children you have to consider patient movement and other things. Here is one company that makes these: Biolase. I think as the cost comes down and the technology improves, you will see these basically replace the dental "drill". The units are expensive. Right now the cost of one of these is up to 50 times the cost of a regular dental handpiece.
How they work is to heat up any water in the area that's zapped till basically it explodes in a little puff. It can be quite precise. Of course, with children you have to consider patient movement and other things. Here is one company that makes these: Biolase. I think as the cost comes down and the technology improves, you will see these basically replace the dental "drill". The units are expensive. Right now the cost of one of these is up to 50 times the cost of a regular dental handpiece.To return to the home page for more info click here: Pediatric Dentistry
Tuesday, August 15, 2006
White Spots On Teeth-Enamel Hypoplasia
When new teeth erupt there may be small (or large) white spots on the teeth. These spots formed during development are called Enamel Hypoplasia or Hypocalcification. The defects in the teeth can be milky white, yellow or brown in color. Sometimes the Enamel, or outer layer of the tooth is even deformed or thin in places. These white or yellow spots are very common. In baby teeth, I tend to see it on the very back molars or the cuspids (the corner teeth). In permanant teeth the first permanent molars are quite commonly affected. Also, the front teeth can be involved leading to cosmetic concerns. You would be surprised how many children have some kind of discoloration. Again, very common.
Hypoplasia can be either a distinct spot on one tooth (sometimes called Turner's tooth, which might have been caused by a trauma or other unknown disturbance to the area during the mineralization of that tooth), or diffuse streaks or cloudy opacities on all the teeth which was some kind of systemic disturbance over a long period of time. Less often, spots are due to Fluorosis, or too much fluoride during development. Usually I cannot pinpoint what causes the hypoplasia, but I can sometimes tell when the disturbance occurred based on the position and appearance of the defect. In fact, sometimes it is in horizontal lines much like layers of brick are on a building. *If the spots were not there when the tooth erupted and have formed recently, they might be the beginning stages of decay.
Treatment: Well, most of the time you don't have to do anything. The areas will not usually decay and, if it isn't a cosmetic problem, we will just observe the area. If the area is more severely affected it might get a cavity or begin to crumble, as the enamel is weaker in those areas. If there is a good bit of breakdown on a back molar, a crown may be needed. If it is just a small spot that is decayed then a small white filling is all that may be needed. Now, for those areas that are on the front teeth with no decay, they just look funny, then there are a few options there too. It all depends on how severe or how deep the lesion is. A technique called Microabrasion, perhaps followed by a little bleaching, can be very useful to treat these cases and make it look at least a little better and it's very easy to do. More severe cases need a white filling or more extensive cosmetic dentistry like a porcelain veneer. With children and teens, I will try the less invasive techniques first. If they need any porcelain work, I usually refer to a cosmetic general dentist when they are finished with braces or around that age.
Mild Hypoplasia:

Moderate Generalized Hypoplasia:

Severe Localized Hypoplasia:

To return to the home page for more info click here: Pediatric Dentistry
Hypoplasia can be either a distinct spot on one tooth (sometimes called Turner's tooth, which might have been caused by a trauma or other unknown disturbance to the area during the mineralization of that tooth), or diffuse streaks or cloudy opacities on all the teeth which was some kind of systemic disturbance over a long period of time. Less often, spots are due to Fluorosis, or too much fluoride during development. Usually I cannot pinpoint what causes the hypoplasia, but I can sometimes tell when the disturbance occurred based on the position and appearance of the defect. In fact, sometimes it is in horizontal lines much like layers of brick are on a building. *If the spots were not there when the tooth erupted and have formed recently, they might be the beginning stages of decay.
Treatment: Well, most of the time you don't have to do anything. The areas will not usually decay and, if it isn't a cosmetic problem, we will just observe the area. If the area is more severely affected it might get a cavity or begin to crumble, as the enamel is weaker in those areas. If there is a good bit of breakdown on a back molar, a crown may be needed. If it is just a small spot that is decayed then a small white filling is all that may be needed. Now, for those areas that are on the front teeth with no decay, they just look funny, then there are a few options there too. It all depends on how severe or how deep the lesion is. A technique called Microabrasion, perhaps followed by a little bleaching, can be very useful to treat these cases and make it look at least a little better and it's very easy to do. More severe cases need a white filling or more extensive cosmetic dentistry like a porcelain veneer. With children and teens, I will try the less invasive techniques first. If they need any porcelain work, I usually refer to a cosmetic general dentist when they are finished with braces or around that age.
Mild Hypoplasia:

Moderate Generalized Hypoplasia:

Severe Localized Hypoplasia:

To return to the home page for more info click here: Pediatric Dentistry
Friday, August 11, 2006
Orthodontic Separators
 When you get braces, the first thing they do is place orthodontic separators. In order to put on orthodontic bands you have to slip them over the teeth like putting a ring on your finger. Teeth are usually tight (it's pretty hard to floss back there isn't it)? So, separators are these little things that are placed between the back teeth to gently move them apart just a little so the bands will fit on easily at your next appointment. In the old days these were metal and used on every tooth because they had to band every tooth. Mostly, however, we use "seps" that are like little rubber bands. The teeth will move apart slowly just a little. It feels like a little piece of food between the teeth. Some kids's teeth get a little sore, but it's not bad. Sometimes after the teeth move, the seps fall out. See your orthodontist or pediatric dentist if you need them replaced prior to your next appointment.
When you get braces, the first thing they do is place orthodontic separators. In order to put on orthodontic bands you have to slip them over the teeth like putting a ring on your finger. Teeth are usually tight (it's pretty hard to floss back there isn't it)? So, separators are these little things that are placed between the back teeth to gently move them apart just a little so the bands will fit on easily at your next appointment. In the old days these were metal and used on every tooth because they had to band every tooth. Mostly, however, we use "seps" that are like little rubber bands. The teeth will move apart slowly just a little. It feels like a little piece of food between the teeth. Some kids's teeth get a little sore, but it's not bad. Sometimes after the teeth move, the seps fall out. See your orthodontist or pediatric dentist if you need them replaced prior to your next appointment.
Sunday, August 06, 2006
Dental Sealants
What can you do to prevent cavities? Well, you can brush, that's good. You can Floss. You can use Fluoridated toothpaste. What else? Dental sealants have been proven to prevent decay in the pits and fissures of teeth. Sealants are usually placed on the first and second permanent molars. You can also seal the bicuspids. You also can seal baby molars, but it is not usually done as the anatomy is different and it can be unnecessarily difficult to work on a very young child just for a sealant. Most kids need sealants, but if the grooves of the teeth are smooth and the child is not cavity prone, I may not recommend it. Oh, adults can benefit from sealants as well, but they are most useful on teeth that are newly erupted, you know, the cavity prone years.
 The idea is to seal up the little grooves, which the brush can't reach. Here is a brush bristle that can't reach down into that really small groove on a molar. Fluoride helps prevent decay as well by strengthening the enamel. Fluoride seems to work best, however, on the smooth surfaces of the teeth. Sealants are for the grooves, so you usually don't use them on front teeth for instance.
The idea is to seal up the little grooves, which the brush can't reach. Here is a brush bristle that can't reach down into that really small groove on a molar. Fluoride helps prevent decay as well by strengthening the enamel. Fluoride seems to work best, however, on the smooth surfaces of the teeth. Sealants are for the grooves, so you usually don't use them on front teeth for instance.
 They are really easy to do. You just sort of paint it on (well, there are several steps, but still fairly easy like using a fiberoptic "flash light") The only thing that can make it harder is if the child has a small mouth or a gag reflex or a wiggly tongue that makes it hard to get back there and keep things dry.
They are really easy to do. You just sort of paint it on (well, there are several steps, but still fairly easy like using a fiberoptic "flash light") The only thing that can make it harder is if the child has a small mouth or a gag reflex or a wiggly tongue that makes it hard to get back there and keep things dry.
 If sealed well, the "cavity bugs" can't get down in there. Sealants last several years and may need to be patched or replaced from time to time. If the kid doesn't chew ice or stuff like that, they will hold up fairly well. If they chip or come off, the "Bugs" can get back in there. My kids have sealants and have never had a cavity!
If sealed well, the "cavity bugs" can't get down in there. Sealants last several years and may need to be patched or replaced from time to time. If the kid doesn't chew ice or stuff like that, they will hold up fairly well. If they chip or come off, the "Bugs" can get back in there. My kids have sealants and have never had a cavity!
Here is another post I made on the same subject:
The American Academy of Pediatric Dentistry recommends placing dental sealants on the first permanent molars (at around 6 years of age) and the second permanent molars (which come in around 12 years of age).
Why? --Well, basically there are a lot of studies that say placing sealants helps reduce the incidence of cavities. Does it mean you will never get cavities?--no, it still can happen, but sealants can reduce the kind of cavities that form in the pits and grooves of the back teeth, you know on the top of the tooth--you still can get them in between the teeth and on the smooth surfaces.
How long do they last?--Even with a well placed sealant I have seen cavities form in areas previously sealed. Sometimes the sealant wears off (chewing ice for instance), or sometimes just because someone is very prone to cavities. They say they last from 5 to 7 years if you take care of them--even adults can get sealants, but they seem to be most effective in the cavity prone years of youth. What is the material? Well, it's basically the same material as used in white fillings without as much filler/reinforcing material, it's a bis-GMA resin, With less filler the sealant can flow into the grooves better. Sometimes we use "flowable" composite which is kind of in between in it's characteristics.
How are they placed? Does it hurt?--I like to say it's like painting fingernails--you basically just paint it on the tooth--now that can be harder than you think as these teeth are in the back of the mouth. Most of the effort is keeping the area dry.
Do you put them on baby teeth?--you can, but generally no. The enamel in baby teeth is different microscopically, they don't seem to stay as well, but sometimes if there is lots of grooves there, so there may be a benefit to placing them. Another thing to think about is that in preschoolers, placing a sealant is just about as difficult as a small filling because little kids, well it's harder to place the sealants. It is often better to simply have regular checkups to catch things early. Also, like I said many cavities in baby teeth are in between the teeth which sealants do not prevent.
I'm going to try and make a video on this some day.

 The idea is to seal up the little grooves, which the brush can't reach. Here is a brush bristle that can't reach down into that really small groove on a molar. Fluoride helps prevent decay as well by strengthening the enamel. Fluoride seems to work best, however, on the smooth surfaces of the teeth. Sealants are for the grooves, so you usually don't use them on front teeth for instance.
The idea is to seal up the little grooves, which the brush can't reach. Here is a brush bristle that can't reach down into that really small groove on a molar. Fluoride helps prevent decay as well by strengthening the enamel. Fluoride seems to work best, however, on the smooth surfaces of the teeth. Sealants are for the grooves, so you usually don't use them on front teeth for instance.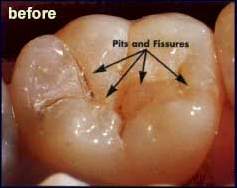 They are really easy to do. You just sort of paint it on (well, there are several steps, but still fairly easy like using a fiberoptic "flash light") The only thing that can make it harder is if the child has a small mouth or a gag reflex or a wiggly tongue that makes it hard to get back there and keep things dry.
They are really easy to do. You just sort of paint it on (well, there are several steps, but still fairly easy like using a fiberoptic "flash light") The only thing that can make it harder is if the child has a small mouth or a gag reflex or a wiggly tongue that makes it hard to get back there and keep things dry.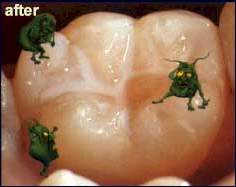 If sealed well, the "cavity bugs" can't get down in there. Sealants last several years and may need to be patched or replaced from time to time. If the kid doesn't chew ice or stuff like that, they will hold up fairly well. If they chip or come off, the "Bugs" can get back in there. My kids have sealants and have never had a cavity!
If sealed well, the "cavity bugs" can't get down in there. Sealants last several years and may need to be patched or replaced from time to time. If the kid doesn't chew ice or stuff like that, they will hold up fairly well. If they chip or come off, the "Bugs" can get back in there. My kids have sealants and have never had a cavity!Here is another post I made on the same subject:
The American Academy of Pediatric Dentistry recommends placing dental sealants on the first permanent molars (at around 6 years of age) and the second permanent molars (which come in around 12 years of age).
Why? --Well, basically there are a lot of studies that say placing sealants helps reduce the incidence of cavities. Does it mean you will never get cavities?--no, it still can happen, but sealants can reduce the kind of cavities that form in the pits and grooves of the back teeth, you know on the top of the tooth--you still can get them in between the teeth and on the smooth surfaces.
How long do they last?--Even with a well placed sealant I have seen cavities form in areas previously sealed. Sometimes the sealant wears off (chewing ice for instance), or sometimes just because someone is very prone to cavities. They say they last from 5 to 7 years if you take care of them--even adults can get sealants, but they seem to be most effective in the cavity prone years of youth. What is the material? Well, it's basically the same material as used in white fillings without as much filler/reinforcing material, it's a bis-GMA resin, With less filler the sealant can flow into the grooves better. Sometimes we use "flowable" composite which is kind of in between in it's characteristics.
How are they placed? Does it hurt?--I like to say it's like painting fingernails--you basically just paint it on the tooth--now that can be harder than you think as these teeth are in the back of the mouth. Most of the effort is keeping the area dry.
Do you put them on baby teeth?--you can, but generally no. The enamel in baby teeth is different microscopically, they don't seem to stay as well, but sometimes if there is lots of grooves there, so there may be a benefit to placing them. Another thing to think about is that in preschoolers, placing a sealant is just about as difficult as a small filling because little kids, well it's harder to place the sealants. It is often better to simply have regular checkups to catch things early. Also, like I said many cavities in baby teeth are in between the teeth which sealants do not prevent.
I'm going to try and make a video on this some day.

Wednesday, July 26, 2006
My Child's First Visit to the Dentist
 The American Academy of Pediatric Dentistry recommends your child's first visit to the dentist be by one year of age or six months after the eruption of the first tooth. "Wow, that's earlier that I thought!"
The American Academy of Pediatric Dentistry recommends your child's first visit to the dentist be by one year of age or six months after the eruption of the first tooth. "Wow, that's earlier that I thought!"I see two year olds every day with tooth decay; sometimes many teeth are involved. If that child had been in our office at age one, we might have limited the damage from the decay. Also, it's a good idea to get them (and you) used to regular visits so that when there is an emergency or other concern the child is used to the office, doctor and staff. Now don't expect a one or two year old to just hop up in the chair and get his teeth cleaned. See here for more info on children's behavior in the office. How Children Behave in the Dental Office, What to Expect.
Here is a good link for additional info on infant oral health care:
Cincinnati Children's Hospital Dental Health Info
Photo courtesy of Quizno's--She's so cute!
Monday, July 24, 2006
Mission Trip to Rio
 Back in 1999, a group from my church went on a misson trip to Brazil. Most of the participants were engineers, houswives, NASA or other government employees, students, etc. I was the only medically related professional to go on this particular trip. Therefore, the objective was not dental or medical treatment. There are such trips organized specifically to serve and treat the poor in various countries while spreading the Gospel. Our particular trip had two main parts. We went to the Methodist camp for children located outside, far outside, Rio DeJaniero, Brazil. Later on, we went into the heart of the favelas (slums) in Rio to a church sponsored school.
Back in 1999, a group from my church went on a misson trip to Brazil. Most of the participants were engineers, houswives, NASA or other government employees, students, etc. I was the only medically related professional to go on this particular trip. Therefore, the objective was not dental or medical treatment. There are such trips organized specifically to serve and treat the poor in various countries while spreading the Gospel. Our particular trip had two main parts. We went to the Methodist camp for children located outside, far outside, Rio DeJaniero, Brazil. Later on, we went into the heart of the favelas (slums) in Rio to a church sponsored school. Way out in the countryside we arrived at the camp. It was September, so it was basically Spring down there. The weather was great. We worked on construction of a new residence building for the kids who came to the camp from Rio. It was one of the few and perhaps only times they would travel outside the city. The building methods were these lightweight clay bricks connected with morter and a wire framework. Much of our time was spent mixing cement, bending wires, lots of digging in the mud, etc. I escaped some of that toil by setting up a mini-dental clinic in one of the other buildings. The kids from the city arrived at the camp about the time we left for Rio. However, children, and some adults, would arrive by foot from the surrounding villages to receive dental treatment. This was done with the help of Evangemed. I spent two days basically removing badly decayed teeth. The mobile van usually used for dental mission trips was temporarily out of commission, so I couldn't do fillings or travel out to the villages. The only thing we could do was extractions. Those of you who have gone on dental mission trips know that most of what you do is extractions anyway. A local physician and dentist from Evangemed were there to do most of the medical stuff. The dentist helped me with some of the dental treatment as well. One evening we went to a local Methodist church service. They do a lot of singing down there and we had to make our contrubution too. We were not prepared for that. I think they may think twice before asking those Americans to sing again! By the way I discovered Guarana down there. It's a ginger-ale like drink made from a bean they have there in the Amazon; really good!
Way out in the countryside we arrived at the camp. It was September, so it was basically Spring down there. The weather was great. We worked on construction of a new residence building for the kids who came to the camp from Rio. It was one of the few and perhaps only times they would travel outside the city. The building methods were these lightweight clay bricks connected with morter and a wire framework. Much of our time was spent mixing cement, bending wires, lots of digging in the mud, etc. I escaped some of that toil by setting up a mini-dental clinic in one of the other buildings. The kids from the city arrived at the camp about the time we left for Rio. However, children, and some adults, would arrive by foot from the surrounding villages to receive dental treatment. This was done with the help of Evangemed. I spent two days basically removing badly decayed teeth. The mobile van usually used for dental mission trips was temporarily out of commission, so I couldn't do fillings or travel out to the villages. The only thing we could do was extractions. Those of you who have gone on dental mission trips know that most of what you do is extractions anyway. A local physician and dentist from Evangemed were there to do most of the medical stuff. The dentist helped me with some of the dental treatment as well. One evening we went to a local Methodist church service. They do a lot of singing down there and we had to make our contrubution too. We were not prepared for that. I think they may think twice before asking those Americans to sing again! By the way I discovered Guarana down there. It's a ginger-ale like drink made from a bean they have there in the Amazon; really good! After our camp experience, we went into the city to spend a couple of nights there. One night there was gunfire nearby. There were also some local pigs, yes pigs, that just roam around--kind of neat. One year a group of Americans had some things stolen from their dorms while they were gone. Word got around the favela and the items were returned right away. The locals knew we were there to help them and they rounded up the kids/teens that took the stuff and made them give it back. As a touristy thing, we went to a cute coastal town and took a boat to a nearby beach and had a great meal at a restaurant on Copacabana beach that evening. Also, we went way up a mountain to the Christ Statue-Amazing!
After our camp experience, we went into the city to spend a couple of nights there. One night there was gunfire nearby. There were also some local pigs, yes pigs, that just roam around--kind of neat. One year a group of Americans had some things stolen from their dorms while they were gone. Word got around the favela and the items were returned right away. The locals knew we were there to help them and they rounded up the kids/teens that took the stuff and made them give it back. As a touristy thing, we went to a cute coastal town and took a boat to a nearby beach and had a great meal at a restaurant on Copacabana beach that evening. Also, we went way up a mountain to the Christ Statue-Amazing!My first thought when I got back was how much "stuff" we have in the U.S. especially our huge houses. It's been a few years since I sent there, but I still miss the people, the strong coffee, the stunning scenery, but I have to say it's good to be home!
 For more info in Mission Trips click here: Evangemed
For more info in Mission Trips click here: EvangemedFor more info click home or here:Pediatric Dentistry
Wednesday, July 12, 2006
Pediatric Dental Office Decor
 Dentists usually hope to have the "dream office" with great decor. If you look at a general dentist office, you will see rich colors, marble counters, adult colors, and modern lighting. It's all to make the patients feel at home, more comfortable. In upscale offices the decor is intended to reflect the high quality of patient care. In pediatric offices it's similar, but the idea is a little different. We do try and have modern everything, but the decor has to cater to the parent (usually mom) and the child. There are play areas, animal pictures, and bright colors. Most pediatric dental offices are well done and have these features to some extent, but usually nothing extreme. Some pediatric offices I have seen are really works of art. Our office (APDA) has a space theme to go along with our community's NASA heritage. We have one of the best around here, expecially our play area.
Dentists usually hope to have the "dream office" with great decor. If you look at a general dentist office, you will see rich colors, marble counters, adult colors, and modern lighting. It's all to make the patients feel at home, more comfortable. In upscale offices the decor is intended to reflect the high quality of patient care. In pediatric offices it's similar, but the idea is a little different. We do try and have modern everything, but the decor has to cater to the parent (usually mom) and the child. There are play areas, animal pictures, and bright colors. Most pediatric dental offices are well done and have these features to some extent, but usually nothing extreme. Some pediatric offices I have seen are really works of art. Our office (APDA) has a space theme to go along with our community's NASA heritage. We have one of the best around here, expecially our play area.You'll see a lot of "open bay" type design in Pediatric and Orthodontic offices with lots of chairs in one big room. We have private operatories as well. If you want a tour of our offices, check out our main web site here APDA. Also, I will try and have more photos on the blog later.
I think the best decorated office I have seen is Dr. Lee Baker's
office in Augusta, Georgia. A long time ago, he visited us at APDA. I guess we scared him off because he decided to go to Alaska for a few years, Ha! After working there, he came back to the South and set up practice in Augusta. Take a look at his office. I have posted a few photos from his web site.



Tooth Internal Resorption
Sometimes the pulp of a tooth gets irritated either by a trauma or a deep cavity and undergoes internal resorption. The cells of the pulp get all "riled" up and the pulp begins to resorb the tooth structure from the inside out. This is sort of like a little pacman eating away any tooth structure in front of it. It's the same process that happens when a new permanent tooth moves up under a baby tooth. Osteoclastic activity slowly begins to dissolve the root of the baby tooth till it's about gone. That's when the baby tooth gets loose. Well, you really don't want that to happen to a tooth from the inside out; especially a permanent tooth. It is rare, but I have seen this most often with baby teeth that have had a history of a large cavity. Most teeth do very well after a restoration, but a few can get internal resorption. It can happen with teeth that have sustained a trauma as well. In a baby tooth, it may not need treatment or it may even need to be removed depending on a lot of factors. It doesn't uaually cause any discomfort. If it's a permanent tooth, it may need a root canal to stop the process as shown here in an x-ray I found on the internet.

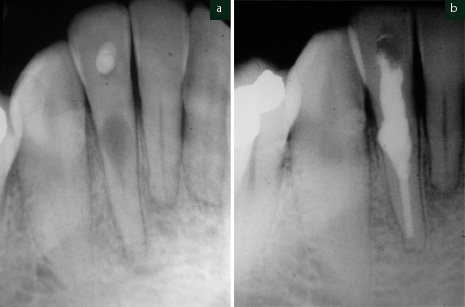
Thursday, July 06, 2006
Fake Baby Teeth (Pedo Partial)
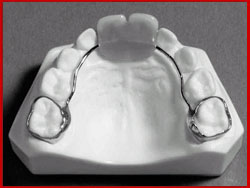 Sometimes a baby tooth gets knocked out or has to be removed due to dental disease. Do you need to replace the missing baby tooth? If the missing tooth is in the back, you will likely need a space maintainer to "hold" the space till the permanent tooth erupts. It's not really a fake tooth but acts like a tooth to hold space. What about that ugly space right there in the front?
Sometimes a baby tooth gets knocked out or has to be removed due to dental disease. Do you need to replace the missing baby tooth? If the missing tooth is in the back, you will likely need a space maintainer to "hold" the space till the permanent tooth erupts. It's not really a fake tooth but acts like a tooth to hold space. What about that ugly space right there in the front?If the missing baby tooth is in the front, you really don't need a space maintainer. Can't you make a partial with a fake tooth on it for looks? Well, you can but you don't have to. There are several types of "Pediatric Partials" to replace knocked out baby teeth. The normal time a front permanent tooth takes to come in varies, but is usually around seven years old. So, if your three year old has lost his tooth early, he will be without something there for about three or four years. Does he care? No, probably not. He can eat and speak just fine even with all four front baby teeth gone. It's us parents that get all bent out of shape over the appearance of the teeth.
These partials are more difficult to do of there is not a lot of room between the gums and the bottom teeth or other related concerns. It is somewhat difficult to take care of these things, but most kids do well. I usually only do these on "cooperative" patients. Keep in mind that kids are rough on their teeth and they are rough on things like this partial. Many times I see the fake teeth get broken off or some other kind of problem. The younger the child the more likely there will be a problem. For these reasons and others, I do not do many "partials" like this.
 Here are a couple of photos of different kinds of pedo partials. You can do one tooth or up to about four teeth. In fact I think it looks better when you have more than one tooth because there is not just one tooth that stands out as being "fake". It is attached to the back baby teeth with orthodontic bands. The partial is removed when the new teeth are ready to erupt.
Here are a couple of photos of different kinds of pedo partials. You can do one tooth or up to about four teeth. In fact I think it looks better when you have more than one tooth because there is not just one tooth that stands out as being "fake". It is attached to the back baby teeth with orthodontic bands. The partial is removed when the new teeth are ready to erupt.Here's one in place (the fake teeth are the upper four middle teeth):

Subscribe to:
Comments (Atom)