It is feared and dreded by all who come in contact with it. It's the pager. When you are a Pediatric Dentist there is one thing we all know about from the first day we started our residency. We were issued some sort of pager that was for after hour’s emergencies. When I was in residency at LSU in New Orleans, I was the recipient of a chunky box, which was an audio pager (ancient by today's standards). This beast would all of a sudden make a loud noise, and then the person on the line by phone would announce what number to call back. At the time it was the Children's Hospital emergency room. You had to listen closely to hear the garbled phone number, but you always knew it was some kind of trauma case that they needed you for. It sent chills up the spine! You knew it meant you would have to travel 30 minutes in the middle of the night to the hospital and deal with some poor child that busted his teeth in some fashion. Oh yes, no assistant to help. In fact I had to open up the dental clinic and turn lots of stuff on and then clean up afterwards and shut it back down. The whole ordeal would last three hours.
I learned that one of the first things to do was turn on the radio otherwise there would be dead silence which is a little unnerving for the child, the distressed parent, and the distressed doctor. Since that time I have learned that every pediatric resident had the same experience across the country. We all get a knowing look on our faces when someone tells of their after hours "pager" experiences.
Now that I am with APDA, we thankfully rotate call. I am on call every fourth week. With a practice this large the number of calls is even greater. The calls tend to fall into one of four categories: Trauma, Tooth Aches, Orthodontic Emergencies like broken wires, and then there are calls like lost separators, erupting teeth, the dreaded tooth just fell out "I think it was a permanent tooth" (it never is) and other milder concerns. Over the years I can sense the level of concern the parent has and can usually deduce what the problem is over the phone. It's always an interesting experience.
There seems to be a pattern as to when people call. There are assorted calls during the weekday evenings, usually nothing that can't wait till the following day. There are the inevitable calls Friday morning and around 5:00, (we are at the hospital most Fridays).
I do fear the calls Saturday and Sunday nights, which are usually traumas, bigger cases, sometimes from the local hospital. Those kinds of calls mean you can't really get too involved with a movie or anything else you can't walk away from. Yes, I have missed the last half of several movies and some church services. Every now and then there is a call in the middle of the night. One was a call at 2:30 am from a young lady from out of town, leaving the next day, that somehow dropped a barbell on her tooth. I had to go in for that one. Needless to say I was tired and grumpy as you might expect. Of course I always try my best to treat each child the best possible way and in a professional manner. It is often the parents that "need the treatment" worse than the child! Even now the sound of the pager going off makes the heart skip a beat.
Friday, December 30, 2005
Friday, December 16, 2005
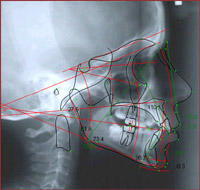
Portable X-Ray?
This blew my mind. Take a look at this new portable hand held battery operated X-Ray head. My first thought when I saw this was, “Wow she will get scatter radiation by standing so close!” Even though the exposure is very very low, dental staff members take many exposures per day. The Alabama guidelines are that you need to stand six feet away from the tube head to be ok. You know, stand outside the room. They say this thing is shielded and you’ll be ok. This device would be really great for overseas mission trips. The web site is www.aribex.com
*More on x-Rays here: Digital X-ray Systems, Wow!


*More on x-Rays here: Digital X-ray Systems, Wow!


Wednesday, November 30, 2005
Aspiring Dentist Saves Christmas!
 News Flash! A soon to be dentist, Hermey (aka Herbie), an elf employed by Santa Claus at the North Pole, has saved Christmas. Evidently Santa’s trip was under threat of cancellation due to inclement weather. Santa was able to make the trip with the assistance of Rudolph the Red Nosed Reindeer. The little known behind the scenes efforts of Hermey made it possible for Rudolph to be available for the trip. The abominable snowman (Bumble) had evidently captured Rudolph and friends.
News Flash! A soon to be dentist, Hermey (aka Herbie), an elf employed by Santa Claus at the North Pole, has saved Christmas. Evidently Santa’s trip was under threat of cancellation due to inclement weather. Santa was able to make the trip with the assistance of Rudolph the Red Nosed Reindeer. The little known behind the scenes efforts of Hermey made it possible for Rudolph to be available for the trip. The abominable snowman (Bumble) had evidently captured Rudolph and friends.  With Rudolph unconscious, Hermey organized a rescue mission with Yukon Cornelius. Upon discovery of the bumble’s real problem, (bad teeth), Hermey with his dental skills, rendered the Bumble a gentle giant. Anesthesia services were provided by Yukon by droping a big rock on the Bumble's head. Rudolph returned unharmed to help guide Santa’s Sleigh! Once again showing the triumph of Dentistry.
With Rudolph unconscious, Hermey organized a rescue mission with Yukon Cornelius. Upon discovery of the bumble’s real problem, (bad teeth), Hermey with his dental skills, rendered the Bumble a gentle giant. Anesthesia services were provided by Yukon by droping a big rock on the Bumble's head. Rudolph returned unharmed to help guide Santa’s Sleigh! Once again showing the triumph of Dentistry.Merry Christmas!
Thursday, November 17, 2005
What’s the tooth fairy’s going rate for baby teeth?

Well, I ask kids all the time what happened to their lost tooth. Most put it under the pillow to get some kind of monetary surprise. Most kids report in the one to five dollar range. (The average is probably one or two dollars with five dollars being common for the first one). I often tell them I used to get 35 cents! Well, one time the “tooth fairy” told me it was kind of dark in there. She placed a five dollar bill under the pillow and retrieved the precious tooth. The next day, it turns out it was so dark, the tooth fairy accidentally had left a $50 bill! That’s the most I have heard so far. Ha..Ha..
Update: I just talked to Dr. Butler this morning (Monday, November 21). He said a $100 bill, which was thought to be a $1 bill, was the most so far he has heard! Wow, the tooth fairy needs some night vision goggles.
Tuesday, November 15, 2005
Katrina Evacuee Update
 Here are a few photos of the LSU School of Dentistry in New Orleans where I did my residency in Pediatric Dentistry. The basement and first floor was flooded and there was 4 feet of water on the main floor. The administration, faculty and students have established facilities in Baton Rouge and around Louisiana. Plans are to return to the New Orleans facility in Spring 2006. I wish them the best of luck. You can get more info on LSU from this site: LSU School of Dentistry
Here are a few photos of the LSU School of Dentistry in New Orleans where I did my residency in Pediatric Dentistry. The basement and first floor was flooded and there was 4 feet of water on the main floor. The administration, faculty and students have established facilities in Baton Rouge and around Louisiana. Plans are to return to the New Orleans facility in Spring 2006. I wish them the best of luck. You can get more info on LSU from this site: LSU School of Dentistry Some the great things this office (APDA) does often are not publicized. Many families displaced from the hurricane have found themselves in the Huntsville area. So far, our office has seen several evacuees from hurricane Katrina. These patients have received treatment at no cost to the family. We wanted to help out these wonderful families that are in a difficult situation right now. The staff organized a drop off site for relief supplies as well. I know we are not the
Some the great things this office (APDA) does often are not publicized. Many families displaced from the hurricane have found themselves in the Huntsville area. So far, our office has seen several evacuees from hurricane Katrina. These patients have received treatment at no cost to the family. We wanted to help out these wonderful families that are in a difficult situation right now. The staff organized a drop off site for relief supplies as well. I know we are not the only ones doing this. I know of several offices in our community that are helping out as well. I am proud to be associated with such a great community and such a great group of professionals. Hopefully these families will be able to go home soon or to establish a new home and a new life here
only ones doing this. I know of several offices in our community that are helping out as well. I am proud to be associated with such a great community and such a great group of professionals. Hopefully these families will be able to go home soon or to establish a new home and a new life here
Tuesday, November 01, 2005
White Fillings vs. Silver Fillings
Who wants silver fillings in their mouth? Some people may, but these days most don’t. Should I have my silver fillings removed? If they are doing well, No! Although silver alloy is still an acceptable material with which to fill teeth, we use only white composite fillings in our office.
Early on, white composite fillings just didn’t hold up as well as the silver ones. Recently, white filling materials have improved enough to compete favorably with silver alloy. Silver fillings do not actually stick or bond to the tooth. Consequently, more tooth structure had to be removed to keep the things from falling out. Composite fillings actually bond to the tooth thus necessitating less removal of tooth structure. They insulate from cold better and act more like a tooth under the stresses of biting. Plus, they just look more natural.
One problem with white fillings is that the technique in placing them can be more exacting. You have to keep the area pretty dry. That can be difficult on a wiggly kid! But hey, we're Pediatric Dentists, we can do anything!
It must be said that once a cavity becomes too large, any kind of filling is not a good idea. In those cases, a crown is needed to cover the whole tooth. --More on that here:
White Crowns For Baby Teeth
Early on, white composite fillings just didn’t hold up as well as the silver ones. Recently, white filling materials have improved enough to compete favorably with silver alloy. Silver fillings do not actually stick or bond to the tooth. Consequently, more tooth structure had to be removed to keep the things from falling out. Composite fillings actually bond to the tooth thus necessitating less removal of tooth structure. They insulate from cold better and act more like a tooth under the stresses of biting. Plus, they just look more natural.
One problem with white fillings is that the technique in placing them can be more exacting. You have to keep the area pretty dry. That can be difficult on a wiggly kid! But hey, we're Pediatric Dentists, we can do anything!
It must be said that once a cavity becomes too large, any kind of filling is not a good idea. In those cases, a crown is needed to cover the whole tooth. --More on that here:
White Crowns For Baby Teeth
Friday, October 28, 2005
Candy Anyone?
 It's Halloween. Parents keep apologizing to me about their kid’s fondness for candy. Everyone thinks dentists are against all candy all the time. Well, let me just say, let the kids have their candy. My kids eat quite a bit around this time of year. All you need to do is use a little common sense. First, avoid the really hard candies; those really can break your teeth, braces or fillings. I've even seen a hard sucker pull off a crown. Second, brush and floss right after you eat the candy. It's not always the quantity of sweets, but how long they stay around. Sugars are the food for the bacteria that cause tooth decay. A cracker that sticks between your teeth and stays there all day and breaks down into sugars is much worse than one sweet that dissolves right away. Of course, a long-term sugar habit is not good for overall health either. Sugarless chewing gum is actually helpful in preventing tooth decay.
It's Halloween. Parents keep apologizing to me about their kid’s fondness for candy. Everyone thinks dentists are against all candy all the time. Well, let me just say, let the kids have their candy. My kids eat quite a bit around this time of year. All you need to do is use a little common sense. First, avoid the really hard candies; those really can break your teeth, braces or fillings. I've even seen a hard sucker pull off a crown. Second, brush and floss right after you eat the candy. It's not always the quantity of sweets, but how long they stay around. Sugars are the food for the bacteria that cause tooth decay. A cracker that sticks between your teeth and stays there all day and breaks down into sugars is much worse than one sweet that dissolves right away. Of course, a long-term sugar habit is not good for overall health either. Sugarless chewing gum is actually helpful in preventing tooth decay.So, eat the sweets (but not too much or you will have some grumpy kids later in the day), then brush and floss. Hey, is that a Milky Way bar over there?
Wednesday, October 05, 2005
When to Call the Dentist, When to Go to the Emergency Room
 Your child just fell riding his bicycle. There is lots of blood. His mouth is a mess. Who do you call? What do you do? Children will find a way to injure themselves despite our best preventive measures as parents. Some orofacial injuries are serious and some are nothing to worry about. How do you tell? Well, here are some guidelines.
Your child just fell riding his bicycle. There is lots of blood. His mouth is a mess. Who do you call? What do you do? Children will find a way to injure themselves despite our best preventive measures as parents. Some orofacial injuries are serious and some are nothing to worry about. How do you tell? Well, here are some guidelines.If there is lots of blood, don't panic. Any injury to the mouth bleeds a lot. Check out the situation; hold a cloth (if you can) with pressure to slow the bleeding. Most bleeding stops within 10 -15 minutes whether you do anything or not. Once your heart stops racing so much and the child is not in such a state, look and see what the problem is. First look and see if there are facial cuts or lacerations, fear of a broken jaw, possible head trauma causing loss of consciousness (concussion), multiple knocked out and displaced teeth (an oral surgeon may need to see you at the hospital), or if you just are not too sure, then you need to go to the ER. They can stitch up any facial lacerations and take major X-Rays to check all that other stuff.
Now, if you don't have those bad things, you still might have a scary mess to deal with. If you go to the ER, you are likely to sit there for two hours and then they will call your dentist anyway. You can call your dentist first and he may be able to save you the trip to the ER.
*If a young child has hit his mouth, there is lots of blood especially on his upper teeth lip area, look and see if it might just be a torn maxillary frenum. That's the little piece of tissue that connects the upper lip to the gum between the two front teeth. If it was tight and gets hit and stretched too much it will tear. It bleeds a lot at first, but will likely be fine after 20 minutes or so. Usually no stitches are necessary. In fact there may be no treatment needed at all. This is a very common injury in preschoolers.
If there is a broken tooth, the ER is not likely to be able to do much. If a tooth is knocked out, and if it is a permanent tooth, you need to get the tooth back in soon as possible, your dentist can help. The ER can put a knocked out tooth back in too, but you still may need a dentist to splint the tooth, so you may want to call the dentist first. If the knocked out tooth is a baby tooth, just leave it out and put it under their pillow. A baby tooth can be intruded (pushed up into the gums) where is is difficult to see. Sometimes it can re-erupt on it's own, but still may need to be removed or need other longer term treatments. If your child is in braces and a wire breaks, etc., call your pediatric dentist or orthodontist.
Here is a useful link for quick reference: APDA Dental Emergencies Quick Reference
More here: Fractured Teeth, Knocked out Teeth, and other Pediatric Dental Accidents
More here: My Child's Tooth is Turning Dark!
Tuesday, September 27, 2005
When is the Best Time to Start Braces?
When we move teeth orthodontically, what happens is that a small pressure exerted over a long period of time stimulates the cells in the bone to resorb in the direction of tooth movement. Once a space is made, the tooth is pushed into the space. Bone fills in behind where the tooth once was located. The process repeats itself again till the tooth is in the final desired position. This process can take place at any age. Yes, you can get braces at 40 years of age! The only caveat is that it usually is easier when the patient is younger. Isn’t most everything? There are however, certain things that can only be done in a growing patient (a preteen or teenager). Once growth ceases, the boney growth of the face halts as well. When a child is growing, certain forces can be applied to guide the growth. That’s usually one of the things a headgear does.

So, when is the best time for my child? Well, it depends on the discrepancy or problem you are trying to correct. If a child has a crossbite, I tend to want to correct it as soon as I see it. I have even corrected a posterior crossbite in a 3 year old! Most of the time braces are not indicated until the patient is between 9.5 and 12 years of age. That’s when a lot of growth takes place. Some children are really ahead of the game in terms of growth. They will get braces sooner. Some patients without severe discrepancies can wait till all their baby teeth fall out around age 12 or so. Different Orthodontists and Pediatric Dentists have different philosophies regarding when to start a particular case. Don’t be surprised if you get a second opinion with a slightly different answer.
I like to see the patient early on so I can guide the eruption of the teeth with early intervention. Placing a lingual arch space maintainer and/or selective removal of certain baby teeth can improve the pattern of tooth eruption. Also, early expansion of a constricted maxillary arch can really help the overall treatment result. One particular case with severe crowding that I remember used timed extractions of baby and then later, permanent teeth. The child ended up not needing any braces at all! So, every child is different. Hey, you know that already.
So, early on, get a Pediatric Dentist or Orthodontist to look examine your child. Most initial crowding problems manifest themselves around 7 years of age when the first permanent teeth are erupting. Good luck, just remember that orthodontics is a long-term proposition. Treatment often takes place over several years. After initial early treatment, you may only be wearing “braces” for 12 to 24 months, but you will wear a retainer once your braces are removed. Oh yes, many of us remember our “retainers”.
More on Braces here: Orthodontic Fashion
Monday, September 12, 2005
Hurricane Katrina and New Orleans

With all the news regarding the Katrina hurricane and the ongoing relief effort, I wanted to comment on my two years spent living in New Orleans during my residency in Pediatric Dentistry at the LSU School of Dentistry. After completing my D.M.D. degree at the Univ. of Alabama, I went to LSU, whose health science programs are in New Orleans, for a two-year residency. In addition to the dental school experience, we spent much time at Children’s Hospital of New Orleans and Charity Hospital. Yes, I remember the theme from “St. Elsewhere” ringing in my ears every time I entered “Charity.” As residents, we assisted with anesthesia on surgery cases of all types as well as doing our own dental OR cases there.
I learned many things in N.O., but most importantly how much Tabasco sauce to put in my gumbo, why there was a plastic baby in the Mardi gras king cake, and how to eat crawfish! Cafe Du Monde in the Quarter has the best café-au-lait and beignets in the world. With all that has happened, I pray all the people of the Crescent City will recover quickly. In fact I know they will!
Once Again,” Laissez les bons temps rouler!”
(Let the good times roll!)
Disclaimer and a note on images, etc.
Disclaimer: Please be aware that I am not trying to practice dentistry over the internet. I am not your dentist (unless of course I am and you are a patient of APDA). In addition, I am probably not licensed in your area, unless your area is Alabama. Please do not ask me any questions that you expect an answer you can be sure of. In other words, I have not seen the patient. I have not seen the x-rays. I have not asked all the right questions and gotten an accurate history to make a diagnosis, etc, etc. I just want this to be a place you can get a little general information, a little view into the profession, and a little entertainment.
Although I have done my best to be accurate and thorough, I do not want anyone to think any information presented here is the best out there, nor do I present our practice or our dentists as any better than any other. In fact, this blog is not a direct part of Alabama Pediatric Dental Associates and Orthodontics. The opinions expressed here are not necessarily those of any of the other doctors or employees of the practice.
I have established this blog in the interest of information and free discussion. Being in Pediatrics means I like to spice up the boring text with pictures and cartoons. All the graphics used are either images made by me, or images thought to be non-copyrighted or intended for public access and are available and viewable on the internet or other public sources. If you see something here that is your work and do not wish it to be used, please let me know. Abusive or crude comments are not allowed. All comments are moderated prior to posting. If you obviously are just trying ot sell something, I may not post your comment. In fact, I reserve the right to post, or not-to-post, any comments made here.
You may see some people used in videos or photos on this blog. Anyone who is identifiable as a patient has signed a consent form giving permission to use his or her images. Here is a good resource if you happened to wonder about: Medical Record Confidentiality HIPAA and Blogging . If I have used your image without your consent and you don't want it on the blog, or if you have changed your mind about the consent given, please let me know right away.
Although I have done my best to be accurate and thorough, I do not want anyone to think any information presented here is the best out there, nor do I present our practice or our dentists as any better than any other. In fact, this blog is not a direct part of Alabama Pediatric Dental Associates and Orthodontics. The opinions expressed here are not necessarily those of any of the other doctors or employees of the practice.
I have established this blog in the interest of information and free discussion. Being in Pediatrics means I like to spice up the boring text with pictures and cartoons. All the graphics used are either images made by me, or images thought to be non-copyrighted or intended for public access and are available and viewable on the internet or other public sources. If you see something here that is your work and do not wish it to be used, please let me know. Abusive or crude comments are not allowed. All comments are moderated prior to posting. If you obviously are just trying ot sell something, I may not post your comment. In fact, I reserve the right to post, or not-to-post, any comments made here.
You may see some people used in videos or photos on this blog. Anyone who is identifiable as a patient has signed a consent form giving permission to use his or her images. Here is a good resource if you happened to wonder about: Medical Record Confidentiality HIPAA and Blogging . If I have used your image without your consent and you don't want it on the blog, or if you have changed your mind about the consent given, please let me know right away.
Disclosure and Contact Info: I do not receive any remuneration or compensation from any companies as a result of any products mentioned or reviewed in this blog, unless specifically noted in the post. I earn my income from treating patients in our private dental practice and related professional activities. I only financially benefit from this blog to the extent that this blog encourages patients to choose our professional dental services in our practice located in Huntsville and Madison Alabama. Office phone: 256-539-7447 Main Office address: 4001 Balmoral Drive, Huntsville, Alabama 35801. Some people have mentioned there is no e-mail contact. I do not wish to place my e-mail online as a lot of junk e-mail tends to accumulate. In addition to the phone and address above, I can be contacted by my twitter account which is linked on the main page. Also, you may leave a comment on this post.
Please do not Plagiarize: All articles are written by me unless otherwise noted, and I hold the content as my own and subject to copyright. As of January 2011 and here forward, all rights are reserved. In the past, I have used the following creative commons copyright:
All materials here created by me are under the Creative Commons Copyright:

Pediatric Dentistry by Dr. Dean Brandon is licensed under a Creative Commons Attribution 3.0 Unported License.
Permissions beyond the scope of this license may be available at http://www.cyberdentist.blogspot.com/2005/09/disclaimer-and-note-on-images-etc.html. Basically, you can share, but give credit as outlined on the Creative Commons Copyright.
There are some photographs or graphics which I do not hold any copyright rights to. As such, they may be used by anyone. Please contact me first if you intend to do so, to make sure it is ok to do so.
This is not a scientific journal, nor is it meant to be a peer reviewed footnoted discourse. This blog, like most blogs, is opinion. If you have a different way of doing things, fine. There is often more than one right way. If you don't like the techniques or methods used, or if you just want to complain, please do so here, but use appropriate discretion. It may just be, however, that you need to get your own blog if you think you have the absolute best way. I have tried to stay within the boundaries of state law and proper ethical standards. I know we're pushing the envelope sometimes with blogging. I hope in the end, this blog makes everyone more informed and a little bit happier. God Bless.
Please do not Plagiarize: All articles are written by me unless otherwise noted, and I hold the content as my own and subject to copyright. As of January 2011 and here forward, all rights are reserved. In the past, I have used the following creative commons copyright:
All materials here created by me are under the Creative Commons Copyright:
Pediatric Dentistry by Dr. Dean Brandon is licensed under a Creative Commons Attribution 3.0 Unported License.
Permissions beyond the scope of this license may be available at http://www.cyberdentist.blogspot.com/2005/09/disclaimer-and-note-on-images-etc.html. Basically, you can share, but give credit as outlined on the Creative Commons Copyright.
There are some photographs or graphics which I do not hold any copyright rights to. As such, they may be used by anyone. Please contact me first if you intend to do so, to make sure it is ok to do so.
This is not a scientific journal, nor is it meant to be a peer reviewed footnoted discourse. This blog, like most blogs, is opinion. If you have a different way of doing things, fine. There is often more than one right way. If you don't like the techniques or methods used, or if you just want to complain, please do so here, but use appropriate discretion. It may just be, however, that you need to get your own blog if you think you have the absolute best way. I have tried to stay within the boundaries of state law and proper ethical standards. I know we're pushing the envelope sometimes with blogging. I hope in the end, this blog makes everyone more informed and a little bit happier. God Bless.
Sunday, September 11, 2005
The Business of Pediatric Dentistry

In the past, most dentists (and pediatric dentists) opened their doors as solo practitioners. Over the years, there has been a shift towards partnerships and group practices. Our practice started when Dr. Charles Hall opened up in the 60’s. Dr. Richard Cannon joined shortly afterwards. Their partnership is near legendary in these parts. (Dr. Cannon is seen above on the left. Dr. Hall is on the right). Dr. Hall eventually became president of the American Academy of Pediatric Dentistry. I joined in 1992 after being in solo practice for a couple of years.

The practice was renamed Alabama Pediatric Dental Associates (APDA). Since then we have added a second office in Madison, Alabama and added three other pediatric specialists and two orthodontists. That necessitated a change in the name again to APDA “& Orthodontics”. Although, we still call it APDA because the whole thing became a mouthful. You can visit our main website with the link on the sidebar. Above you can see us opening our new Huntsville office with Huntsville Mayor Loretta Spencer.
Our staff has grown as well. I often wonder how we keep our sanity working with around 40 women! With such a large practice, management and the business aspects of the profession become more important and certainly demand more time. We know all about patient treatment, but are ill equipped initially to understand the business of dentistry. Often we say, “ I don’t care about all that, just let me treat the patients”. However, we soon find out if you can’t stay in business, you can’t offer the best treatment for your patients. Like it or not, these days you must understand business.
Our doctors and management meet often on business and patient issues. We also meet annually with our accounting firm Cain, Watters, and Associates, P.C. in Dallas about once per year. They helped us with transitioning in our new dentists to the practice.
In addition to the intensive education to become a dentist and the continuing educational requirements to keep up with current techniques, etc., there is the real need for business and management skills development. Just look at some of the following things you need to master, but never really get much in dental school:
Hiring personnel, government regulations such as OSHA and HIPPA, licenses, tax laws, supplies and inventory management, financing and banking, employee benefits, bonuses, pension plans and pension law, long range planning, and practice transitions. By the way, have I mentioned anything about patient treatment? We are just scratching the surface here. I’ll add more regarding these topics and more especially including our wonderful patients and their dental care.
If you want more, go back to the home page or click here:Pediatric Dentistry
Wednesday, September 07, 2005
How do you become a Pediatric Dentist or Orthodontist?
What does it take to become a Pediatric Dentist or Orthodontist?
In addition to being the right kind of person, patient, smart, kind, good manual dexterity, and good people skills, it requires, well, lots of schooling. I often run into people who assume dental school is sort of a trade school you do after high school for a couple of years. In fact most dentists must complete a 4-year university degree before even entering dental school. Dental school is at least 4 years. At that point you may want to put out your shingle and start practice. You receive either a DDS, doctor of dental surgery, or a DMD, doctor of dental medicine. I am not going to go into it here, but suffice it to say there is no substantive difference between these two degrees, especially as far as the patient is concerned.
Most dentists go on for further schooling! Many do a general practice residency in a hospital setting to refine their skills. Some go on to obtain a PhD for a career as an educator or in research. Some obtain an MD degree in addition to their DMD or DDS. Many do, as I did, and specialize in one of the recognized dental specialties: Oral and Maxillofacial Surgery, Orthodontics, Pediatric Dentistry, Endodontics, Periodontics, Prosthodontics, Oral Pathology, Oral Radiology, or Public Health. Most of these require at least two additional years of intense study. I’ll have more on these specialties later.
Let’s see, that’s at least ten years after high school to become a Pediatric Dentist or Orthodontist! Not exactly the local trade school.
*February 10, 2006 Update: check out this new post on this topic The Dental Specialties
If you want more, go back to the home page or click here:Pediatric Dentistry
In addition to being the right kind of person, patient, smart, kind, good manual dexterity, and good people skills, it requires, well, lots of schooling. I often run into people who assume dental school is sort of a trade school you do after high school for a couple of years. In fact most dentists must complete a 4-year university degree before even entering dental school. Dental school is at least 4 years. At that point you may want to put out your shingle and start practice. You receive either a DDS, doctor of dental surgery, or a DMD, doctor of dental medicine. I am not going to go into it here, but suffice it to say there is no substantive difference between these two degrees, especially as far as the patient is concerned.
Most dentists go on for further schooling! Many do a general practice residency in a hospital setting to refine their skills. Some go on to obtain a PhD for a career as an educator or in research. Some obtain an MD degree in addition to their DMD or DDS. Many do, as I did, and specialize in one of the recognized dental specialties: Oral and Maxillofacial Surgery, Orthodontics, Pediatric Dentistry, Endodontics, Periodontics, Prosthodontics, Oral Pathology, Oral Radiology, or Public Health. Most of these require at least two additional years of intense study. I’ll have more on these specialties later.
Let’s see, that’s at least ten years after high school to become a Pediatric Dentist or Orthodontist! Not exactly the local trade school.
*February 10, 2006 Update: check out this new post on this topic The Dental Specialties
If you want more, go back to the home page or click here:Pediatric Dentistry
What is Pediatric Dentistry?
I have started this blog primarily for those interested in Pediatric Dentistry and Orthodontics. Pediatric Dentistry is a specialty of dentistry involving comprehensive dental care for children from birth to age 21. We also see patients older than 21 if they have special needs such as cerebral palsy or Down's syndrome. Part of Pediatric Dentistry is providing orthodontics or "braces". Alabama Pediatric Dental Associates and Orthodontics is the practice with which I am affiliated. We provide comprehensive dental treatment for children and also have an orthodontist on staff for most of the comprehensive orthodontic cases. I work there most days and will try to comment here when I can.
If you have something constructive to say, please do. If you have a concern, let us know as well. God Bless!
Children's Dentistry-a few more details about what we do
If you want more, go back to the home page or click here:Pediatric Dentistry
If you have something constructive to say, please do. If you have a concern, let us know as well. God Bless!
Children's Dentistry-a few more details about what we do
If you want more, go back to the home page or click here:Pediatric Dentistry
Subscribe to:
Posts (Atom)